A recent New York Times headline stated “Children born by cesarean section may have important differences that affect their neurodevelopment”, based on a recent JAMA article1. The neurodevelopmental outcomes that were correlated were autism and attention deficit disorder.
The article goes on to explain that this is an association not a cause, and that conditions requiring a Cesarean section could cause the association, rather than the procedure itself. The article is a meta-analysis and does not subgroup Cesarean sections, for example, those done for non-reassuring fetal heart tracings. I think this is an important piece of missing data. My concern is that experimental evidence has demonstrated that very minimal hypoxic stress to a pregnant animal can cause pontosubicular neuronal necrosis in the fetus. I will discuss the specifics of the lesion below, but the importance is that relatively mild episodes of hypoxia/ischemia in the infant brain can cause loss of specific groups of neurons. In the typical sheep experiment, this lesion occurs after just 10 minutes of complete umbilical cord occlusion2-4. It is not a stretch to suggest that some of the infants undergoing emergency Cesarean sections have equivalent episodes of hypoxia.
Pontosubicular neuronal necrosis is a pathological lesion in which individual neurons in the basis pontis and in the subiculum show karyorrhexis (breaking apart) of the cell nucleus. In both experimentally produced lesions and in autopsy tissue, the karyorrhectic neurons demonstrate evidence of apoptosis5-8. These neurons are responding to the hypoxic event with basically programmed cell death, or as sometimes put, cell suicide. The cell death is not the direct result of hypoxia or acidosis. As discussed in my blog pages on primate models and particularly on Ron Myers model, neuronal necrosis occurs in a stereotyped pattern of progressively recruited areas of the brain the longer the infant monkey is completely hypoxic. This is a different pattern from the extensive coagulation necrosis seen in the white and gray matter with partial hypoxia. This latter pattern is typical of cerebral palsy. Myers proposed that the sequence of areas reflected damage starting with the most metabolic active areas progressing to less active areas. These studies evaluated neuronal necrosis starting at 14 minutes of total asphyxia, and did not include pontosubicular necrosis, but the appearance of the more advanced lesions is very similar to those in the pons and subiculum.
As a pathologist, I have often seen pontosubicular necrosis in stillborn infants in which an anatomic cause of death was not found (Fig 1).
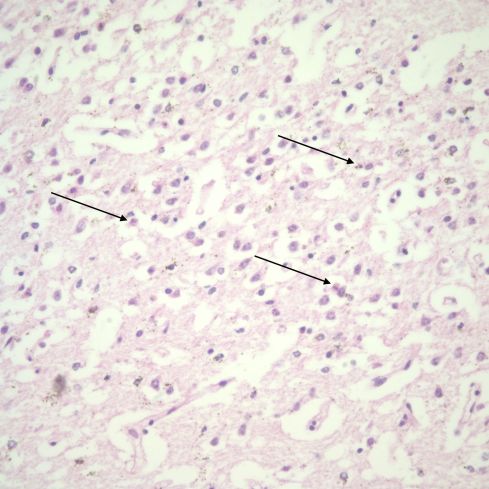
This photomicrograph from the region near CA1 of the hippocampus shows numerous karyorrhectic neurons (arrows) H&E 40x
In these cases it is not unreasonable to speculate that the lesion reflects as recurrent or persistent hypoxic event prior to the final lethal event. Others have published on the finding of neuronal necrosis in stillbirth9,10. Since even apoptosis takes time, the lesion was not likely the result of the immediate episode that caused death. Interestingly, the lesion is found in neonates with more chronic causes of hypoxic (and hyperoxic) episodes and must be part of an ongoing process11. The dead cells are then removed without inflammation or scarring. The scattered, necrotic, cells that I see as a pathologist would not be detectable by the usual clinical imaging techniques. We simply have no way of knowing if pontosubicular necrosis has occurred in a living infant.
It is unclear if neurons are later replaced after pontosubicular necrosis or if a specific population of cells is permanently reduced. In my examination of the slides, the karyorrhectic cells appear to be in Sommer’s sector (CA1) of the hippocampus, the anatomic area adjacent to the subiculum, but I am not a neuropathologist, and the brains are very small. In either location, this is an area that appears to be important in correlating positional information with other cues12. Its role in memory and emotion is likely complex. Uncal lesions in the monkey brain lead to a lack of response to social cues (The uncus is in physical continuity with the hippocampus.)13. A reasonable hypothesis is that loss of certain neurons could influence attention and response to environmental clues. Mostly as an aside, the evolutionary basis if any of cell apoptosis in the developing brain to hypoxic stimuli is curious, but we know that the developing brain is in some sense a competitive environment for neurons, and perhaps apoptotic pathways may be hijacked by the external fetal hypoxic event.
The importance of noting the risk of subtle neuronal necrosis is important. If neuronal necrosis is causing neurodevelopmental disease with relatively mild fetal hypoxia, then anti-apoptotic therapy may be better. In the experimental worm, C. elgans mutations of the insulin/ insulin growth factor homolog DAF-2 can help prevent apoptosis 14. Identifying similar mutations in humans that could influence susceptibility to neuronal necrosis might allow more aggressive obstetrical care. More information on the mechanism and outcome of pontosubicular necrosis is needed. Further investigation of subtle neuronal necrosis following brief fetal hypoxia may provide insight into one possible lesion for a link between Cesarean section and neurodevelopmental pathology of autism and attention deficit.
References:
- Zhang T, Sidorchuk A, Sevilla-Cermeno L, et al. Association of Cesarean Delivery With Risk of Neurodevelopmental and Psychiatric Disorders in the Offspring: A Systematic Review and Meta-analysis. JAMA Netw Open 2019;2:e1910236.
- Mallard C, Gunn A, Williams C, Johnston B, Gluckman P. Transient umbilical cord occlusion causes hippocampal damage in the fetal sheep. Am J Obstet Gynecol 1992;167:1423-30.
- Keunen H, Deutz NE, Reempts JL, Hasaart TH. Transient umbilical cord occlusion in late-gestation fetal sheep results in hippocampal damage but not in cerebral arteriovenous difference for nitrite, a stable end product of nitric oxide [In Process Citation]. J Soc Gynecol Investig 1999;6:120-6.
- Fujii EY, Takahashi N, Kodama Y, Roman C, Ferriero DM, Parer JT. Hemodynamic changes during complete umbilical cord occlusion in fetal sheep related to hippocampal neuronal damage. Am J Obstet Gynecol 2003;188:413-8.
- Rossiter JP, Anderson LL, Yang F, Cole GM. Caspase-3 activation and caspase-like proteolytic activity in human perinatal hypoxic-ischemic brain injury. Acta Neuropathol 2002;103:66-73.
- van Landeghem FK, Felderhoff-Mueser U, Moysich A, et al. Fas (CD95/Apo-1)/Fas ligand expression in neonates with pontosubicular neuron necrosis. Pediatr Res 2002;51:129-35.
- Stadelman C, Mews I, Srinivasan A, Deckwerth TL, Lassmann H, Bruck W. Expression of cell death-associated proteins in neuronal apoptosis associated with pontosubicular neuron necrosis. Brain Pathol 2001;11:273-81.
- Takizawa Y, Takashima S, Itoh M. A histopathological study of premature and mature infants with pontosubicular neuron necrosis: neuronal cell death in perinatal brain damage. Brain Res 2006;1095:200-6.
- Mito T, Kamei A, Takashima S, Becker LE. Clinicopathological study of pontosubicular necrosis. Neuropediatrics 1993;24:204-7.
- Grafe MR, Kinney HC. Neuropathology associated with stillbirth. Semin Perinatol 2002;26:83-8.
- Ahdab-Barmada M, Moossy J, Painter M. Pontosubicular necrosis and hyperoxemia. Pediatrics 1980;66:840-7.
- Bilkey DK. Neuroscience. In the place space. Science 2004;305:1245-6.
- Dicks D, Myers RE, Kling A. Uncus and amiygdala lesions: effects on social behavior in the free-ranging rhesus monkey. Science 1969;165:69-71.
- Scott BA, Avidan MS, Crowder CM. Regulation of hypoxic death in C. elegans by the insulin/IGF receptor homolog DAF-2. Science 2002;296:2388-91.

Leave a comment