Explanation of the selected name:
The “chronic” refers to the type of inflammatory cell, not to the duration of the lesion nor to a necessarily slow onset. The lesion is characterized by the accumulation of blood monocytes/histiocytes, hence a chronic inflammatory pattern. These monocytes are in maternal blood not in tissue, but the consensus is to refer to them as histiocytes. The monocytes are maternal, although testing of this origin is seldom done. The name implies that the accumulation of the inflammatory cells is in the placental intervillous space. The consensus differential diagnosis separates this entity from intervillous monocyte accumulations initiated by a specific infectious agent such as malaria, or rarely CMV. This does not preclude that the origin of CHIV may be from the sensitization to a paternal antigen, which could be a different antigen in different groups of cases, or that the origin may be an autoimmune antigen in patients with a genetic or acquired tendency to autoantibodies.
Other Search Terms1:
Chronic Massive Intervillositis
Intervillositis
Perivillous Histiocytosis
Intervillities
Indicators for placental examination:
Fetal Growth Restriction
Intrauterine Fetal Death
Maternal history of intervillositis or recurrent fetal loss
Spontaneous abortion/fetal loss at any gestation
History of the lesion
Early reports: The earliest report of intervillositis as a separate entity is probably a report in German from 1972, cited in the Benirschke and Kauffman textbook 19952. Intervillous monocytes were described by Russell in 1980 as a component of villitis3. The first published paper in English describing “massive chronic intervillositis” was in 1987 by Labarrere and Mullen4. I recall a presentation of a case by Dr. Eugene Perrin at an SPP/CAP meeting at which the participants had not seen the lesion before, and this was followed at a later date by a presentation of “massive chronic intervillositis to the SPP by Dr. Valderrama in 19925. The next publication of 6 cases, not all massive, was by Jacques and Qureshi in 1993 entitled “Chronic intervillositis of the placenta”6. The lesion was subsequently reported by others in a series of patients with fetal loss including maternal recurrence by Salafia et. al. and Redline et.al7-9. In 2000, Boyd and Redline published a paper entitled “Chronic histiocytic intervillositis: a placental lesion associated with recurrent reproductive loss10. By the end of the 1990’s intervillositis had been associated with early fetal loss, fetal growth restriction, recurrence in subsequent pregnancies and with autoimmune disease.
Association with autoimmunity: Perhaps the first report of recurrence of the lesion was by Doss et.al. in 1995 in a patient with a history of abnormal antibodies, and who had an apparent benefit with prednisone therapy during the pregnancy11. The patient also had elevated maternal serum alpha fetal protein levels. Salafia and Cowchock reported in 1997 that 4 of 16 fetal losses before 18 weeks of gestation demonstrated chronic intervillositis in women who subsequently had anti-phospholipid antibodies identified12.
Infectious causes: In the 1990’s, the lesion was identified in the placenta of patients with malaria, by Leopardi et. al. and Ordi et. al13,14. Hyde and Benirschke also reported an intervillositis with acute inflammatory cells in gestational psittacosis15. These cases raised the possibility that some chronic intervillositis might be associated with infections that circulated in the blood such as Babesiosis or Ehrlichosis, but there has been no published evidence of this.
Paternal alloantibody: I am not sure who first speculated that chronic intervillositis could be due to an antibody response to paternal antigens on fetal villi, but this idea was probable from the recurrence of the lesion. This idea supports earlier studies of Faulk et. al. into secondary aborters, that is mothers who have had a normal first pregnancy but then have recurrent fetal loss. This pattern is in some ways analogous to Rh allo-immunization. This group proposed the existence of human trophoblast-lymphocyte cross reactive antigens as a new system of alloantigens. They suggested that unique trophoblastic lactoferrin epitopes could produce monocyte activation.
Relationship to villitis and fibrinoid: From the earliest papers, there was speculation and confusion about the relationship of the lesion to lymphocytic/chronic villitis and to perivillous fibrinoid deposition. In the Benirschke Kauffman textbook 1995, figure 436 related to the discussion of the Jacques and Qureshi paper shows intervillositis associated with severe villitis2. In 1998, Jacques and Quereshi reported 2 cases of chronic chorioamnionitis with intervillositis16. Subsequent case series have confirmed the association of intervillositis with villitis and perivillous fibrinoid deposition.
Diagnostic Features
Gross: No specific features reported, but the placenta is often small for gestational age, and may show increased perivillous fibrinoid.
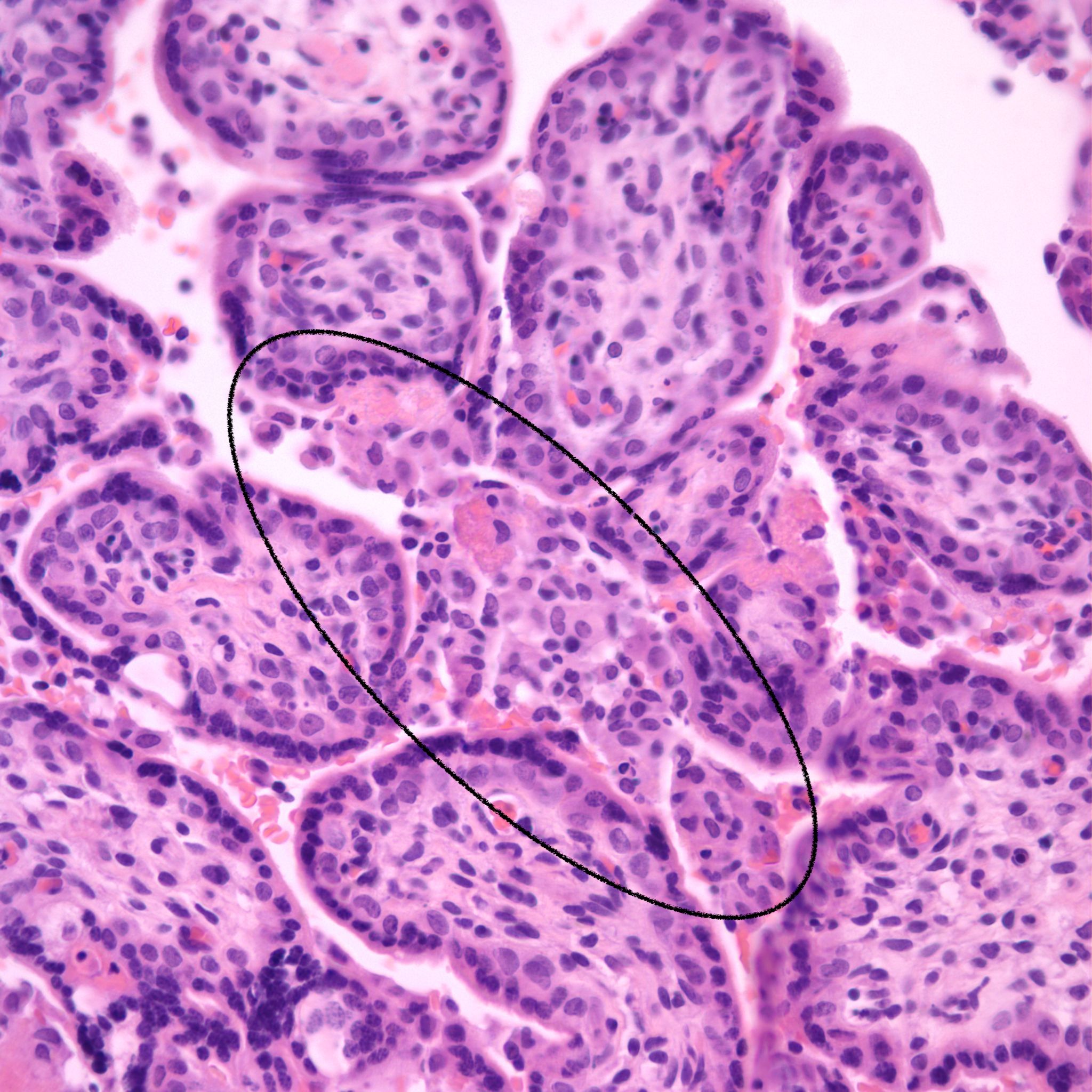
Microscopic criteria: The primary criterion is monocytes clustered in the intervillous space which can be confirmed by CD 6810,17. The monocytes often have kidney bean shaped nuclei and prominent cytoplasm. Some other consensus criteria are that the inflammatory cells in the intervillous space should be at least 80% monocytes, and these should be maternal cells1,17.
Extent and Severity: If this is an untreated case, one accepted criterion is that the monocytes occupy 5% of the sampled intervillous space. The severity can also be graded usually as less than versus more than 50% of the intervillous space filled with monocytes. The number of monocytes in the largest clusters, and whether the distribution is evenly distributed or focal may also be useful observations.
After identification of monocytes:
a) The mother should have a normal blood count without increased monocytes from malignancy, EBV infection.
b) Look at maternal red cells for evidence of malaria or other blood microorganism. Malaria is the only reported infection thus far.
c) Examine any other specimens of fetal loss or placenta from the mother to find intervillositis.
If monocytes fill less than 5% of the intervillous space: If the mother has had a previous pregnancy with this lesion (note any treatment with the current pregnancy), the fetus or infant is small for gestational age, or there is a history of recurrent fetal loss, then, the diagnosis should be considered as possible, not proven.
Other associated pathology
Perivillous fibrinoid: See entry on perivillous fibrinoid. See pathogenesis below. Some perivillous fibrinoid is a normal finding especially in the subchorionic intervillous space, along septa and adjacent to infarctions. Currently, there are no specific criteria to identify perivillous fibrinoid that is a consequence of syncytiotrophoblast injury from intervillositis. Increased perivillous fibrinoid above normal has been associated with CHIV.
Villitis of Unknown (A)Etiology (VUE): See entry on villitis of unknown aetiology, and pathogenesis below. As with perivillous fibrinoid, the relationship of VUE to the intervillositis is still not understood. Villitis of unknown aetiology villitis, if independent of intervillositis, would be present in the same percentage of cases as in the general population, around 6%. There is both observational evidence and potential pathogenetic relationships between villitis and intervillositis. An association of the two lesions is probable.
Ancillary staining of the specimen:
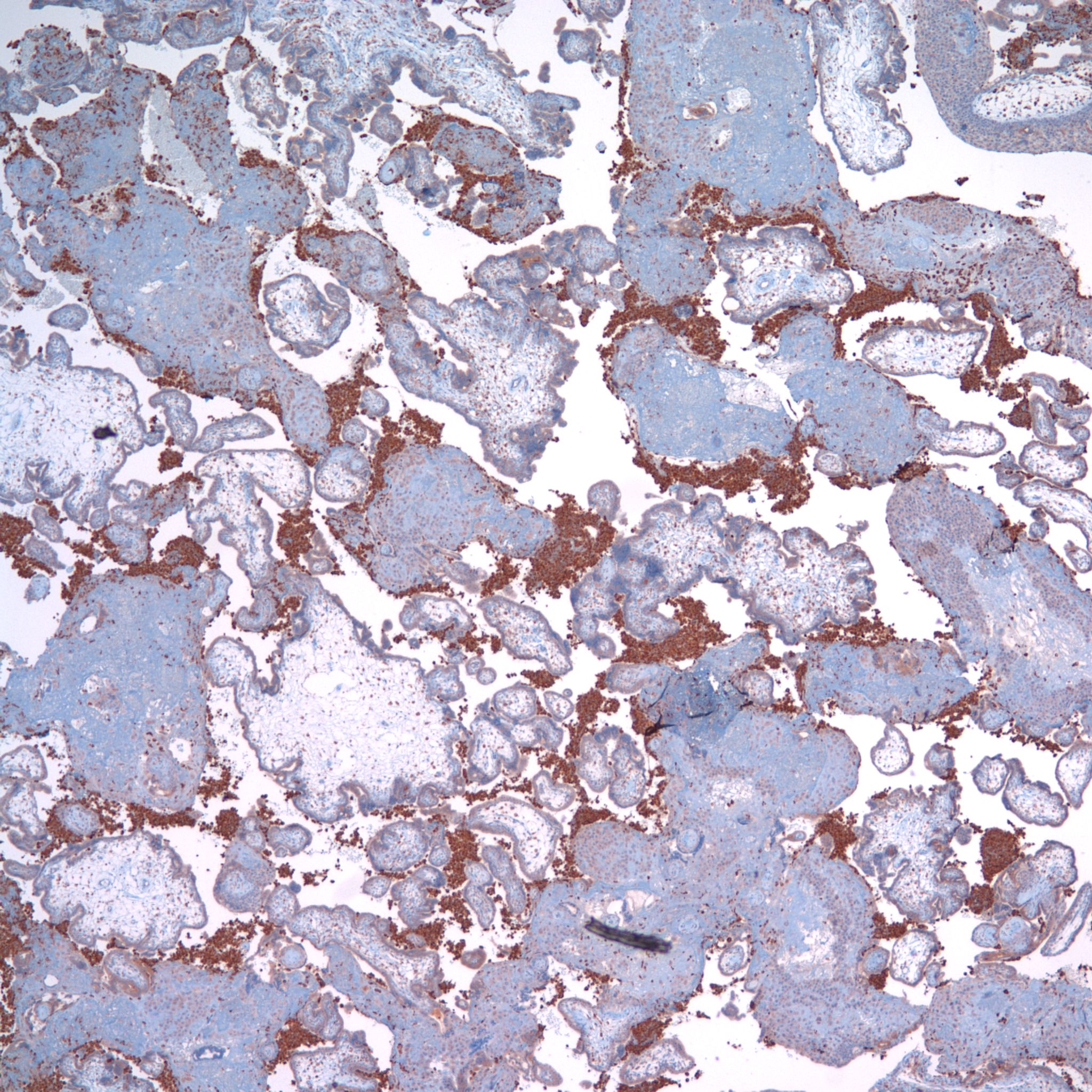
CD68 or alkaline phosphatase: to confirm that the intervillous cells are monocytes, but is not required for meeting the diagnostic criteria
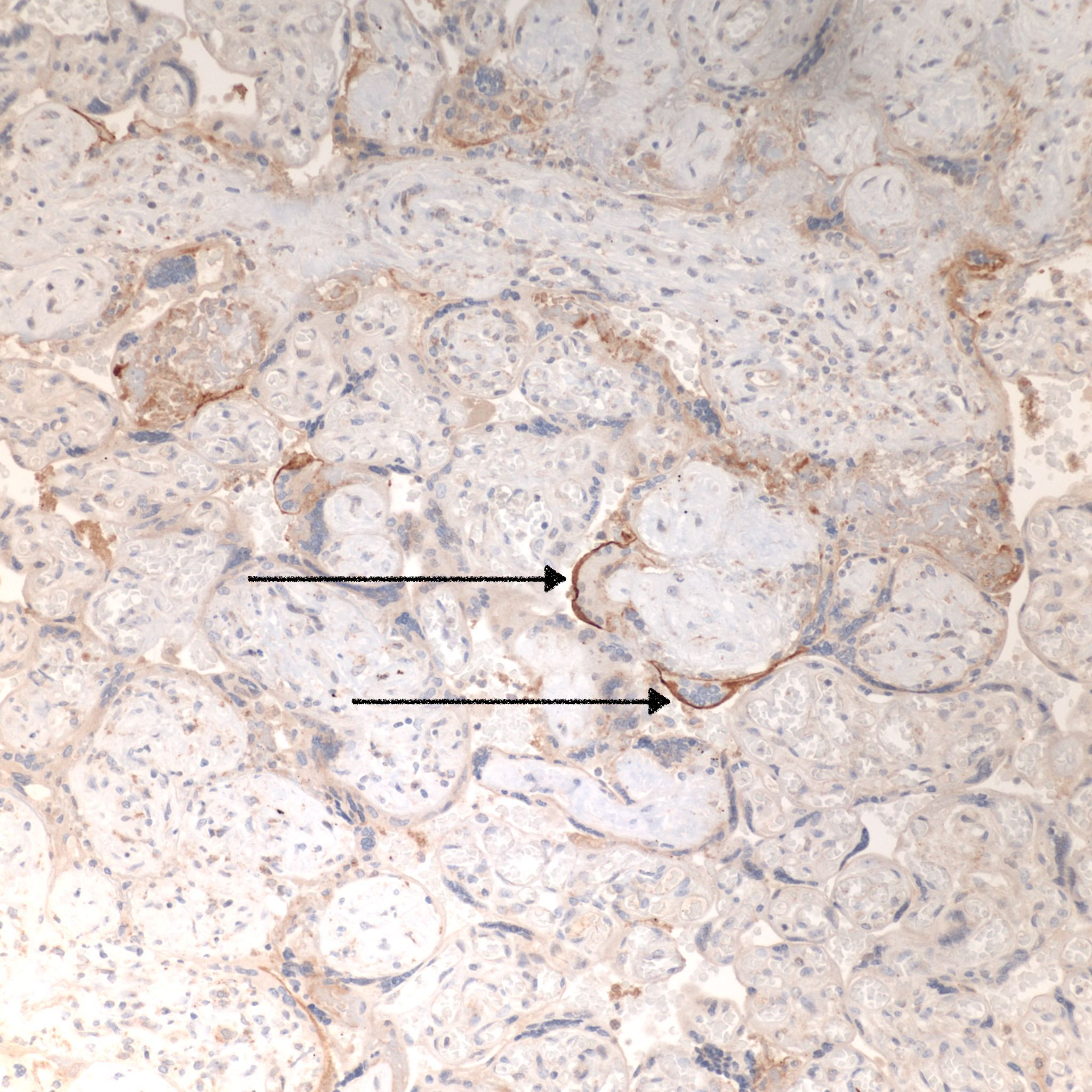
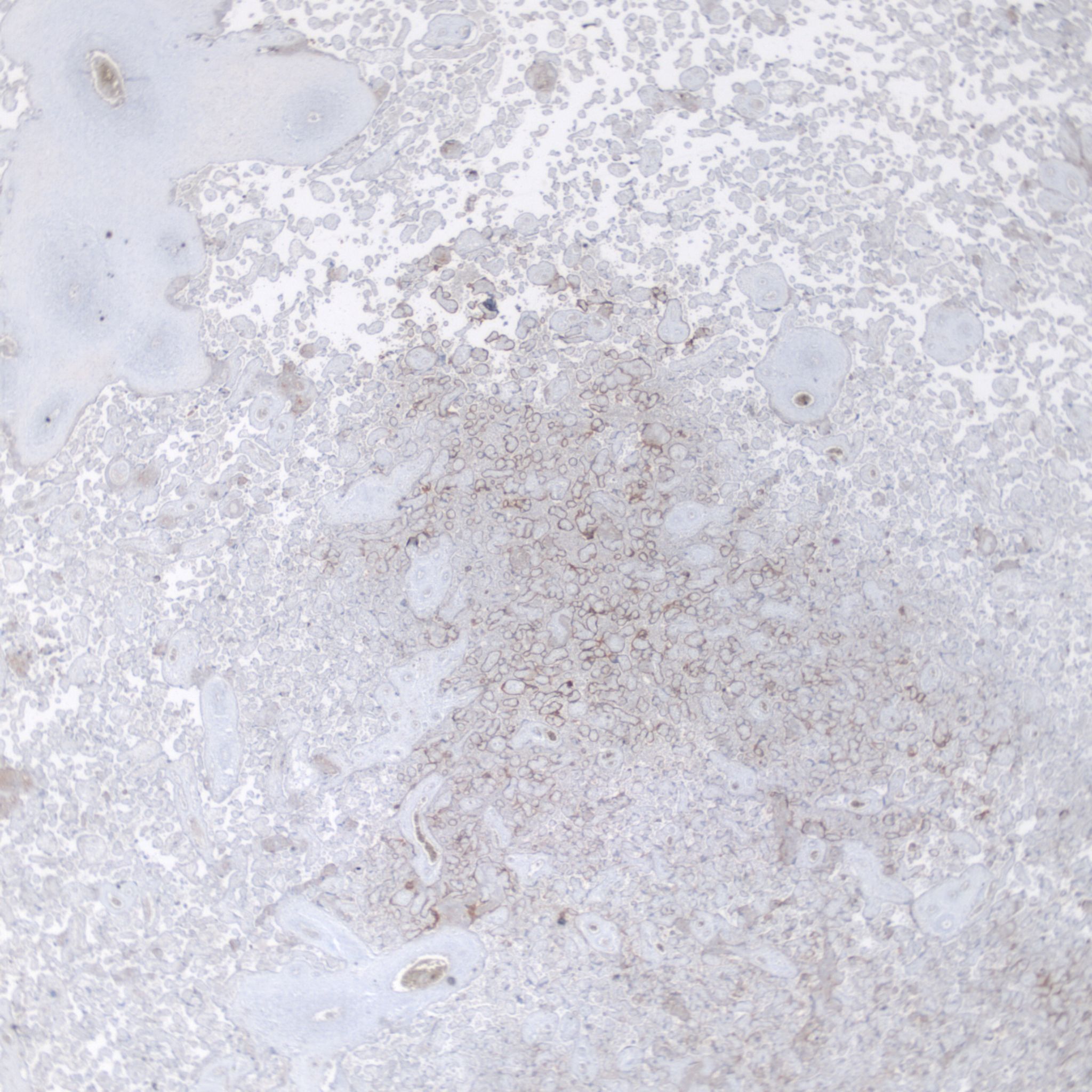
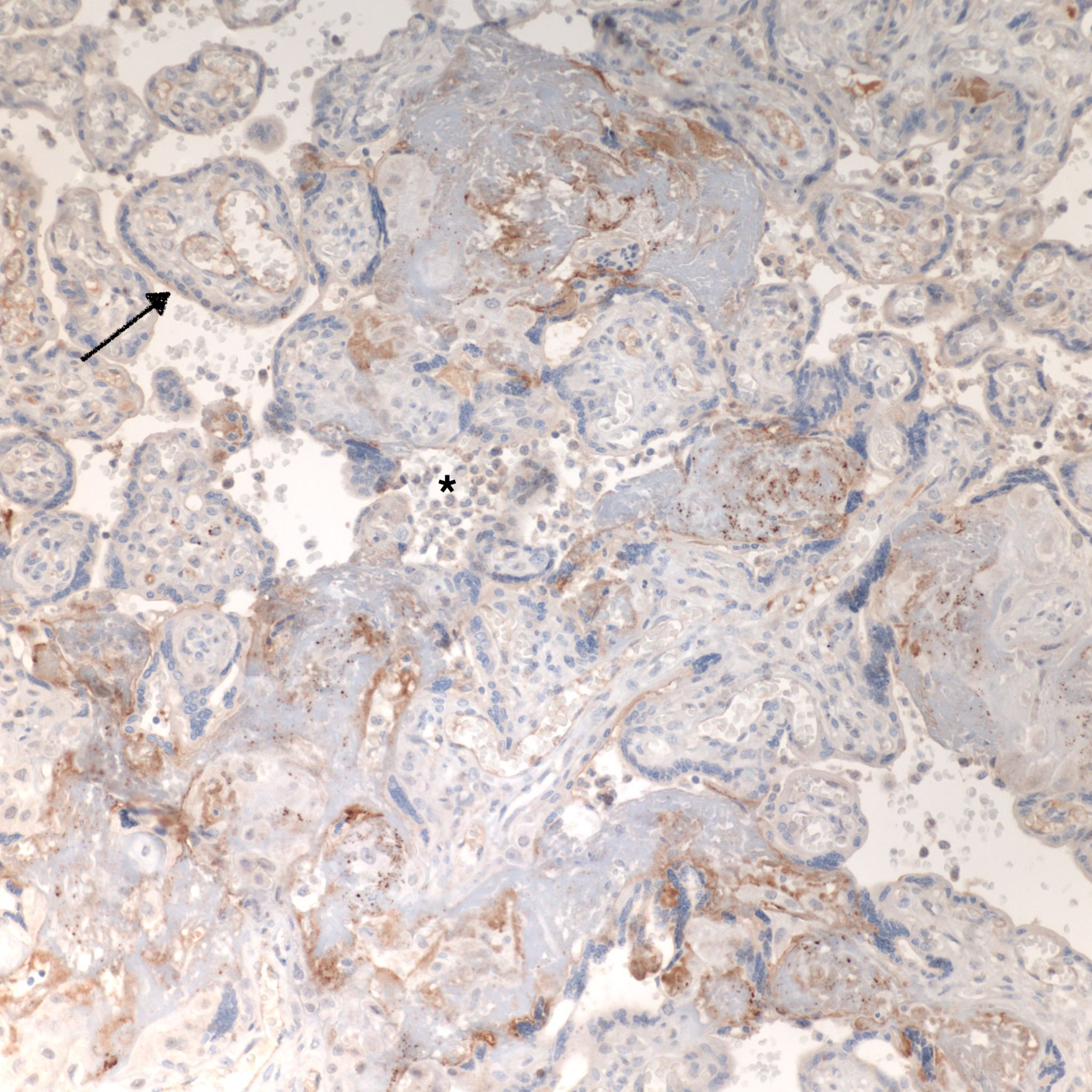
C4d: to show evidence of complement fixation on the microvillous surface of the syncytiotrophoblast. While further study is needed, the subclassification of intervillous monocyte accumulations into those with and without complement fixation and the subclassification of villitis of unknown aetiology with intervillous monocytes into those with and without complement fixation may prove to be a useful distinction.
C4d: One study of CHIV compared 3 histologic groups of placentas demonstrating intervillous histiocytes: Few intervillous monocytes, massive intervillous monocytes, and intervillous monocytes associated with villitis of unknown aetiology18. Each group was further divided into subcategories based on the extent of c4d immunostaining of the microvillous surface of the syncytiotrophoblast. The outcome variables were fetal death or growth restriction. In the analysis, without a formal ROC study, it appeared that staining less than 25% of the villous surface was a natural cut off point from greater than 25%. As can be seen in the Table 1 of the raw data, that with rare exceptions, all the cases with less than 25% of c4d trophoblast staining, and often without any staining, were either associated with few intervillous monocytes, or with villitis. Fetal death or growth restriction was almost always associated with more than 25% of the villous surface stained with c4d. The lack of statistical significance in the comparisons is likely due to small sample size.
| Case | C4d | GA: weeks | days | b.w. | SB | SGA | recurrent | G | T | P | A | L | histology | |
| 1 | 3 | 40 | 0 | 1506 | 1 | 1 | 3 | 2 | 0 | 0 | 2 | MCI | ||
| 2 | 3 | 27 | 230 | 1 | 1 | W | MCI | |||||||
| 3 | 3 | 28 | 2 | 311 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | MCI | ||
| 4 | 3 | 23 | 4 | 815 | 1 | 0 | Z | MCI | ||||||
| 5 | 3 | 38 | 2061 | 0 | 1 | 5 | 3 | 1 | 1 | 4 | MCI focal | |||
| 6 | 3 | 40 | 4 | 3010 | 0 | 0 | 3 | 1 | 0 | 1 | 1 | FIM | ||
| 7 | 3 | 37 | 4289 | 0 | 0 | 2 | 0 | 1 | 0 | 1 | VIM | |||
| 8 | 3 | 39 | 2937 | 0 | 0 | 3 | 0 | 1 | 1 | 1 | MCI | |||
| 9 | 3 | 34 | 1720 | 0 | 0 | Z | 11 | 0 | 1 | 9 | 1 | MCI | ||
| 10 | 3 | 30 | 1230 | 0 | 0 | 2 | 0 | 0 | 1 | 0 | VIM | |||
| 11 | 2 | 26 | 314 | t | 1 | 1 | 0 | 0 | 0 | 0 | FIM | |||
| 12 | 2 | 22 | 270 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | MCI | |||
| 13 | 2 | POC | 1 | 0 | X | 6 | 0 | 1 | 4 | 1 | MCI | |||
| 14 | 2 | 34 | 0 | 1640 | 1 | 0 | 4 | 2 | 0 | 1 | 1 | VIM | ||
| 15 | 2 | 33 | 4 | 1505 | 0 | 0 | 3 | 0 | 0 | 2 | 0 | VIM | ||
| 16 | 2 | 37 | 3 | 2710 | 0 | 0 | 3 | 2 | 0 | 1 | 1 | MCI focal | ||
| 17 | 2 | 38 | 4 | 2770 | 0 | 0 | 3 | 2 | 0 | 0 | 2 | VIM | ||
| 18 | 2 | 2750 | 0 | 0 | 3 | 3 | 0 | 0 | 2 | MCI focal | ||||
| 19 | 2 | 34 | 5 | 0 | 0 | 3 | 2 | 0 | 0 | 2 | VIM | |||
| 20 | 2 | 16 | 5 | x | 1 | x | Z | MCI | ||||||
| 21 | 2 | 33 | 3 | 1536 | 1 | 0 | 2 | 1 | 1 | 0 | 1 | VIM | ||
| 22 | 2 | 27 | 2 | 1454 | 0 | 0 | 2 | 0 | 1 | VIM-CMV | ||||
| 23 | 1 | 27 | 2 | 312 | t | 1 | V | 3 | 2 | 0 | MCI | |||
| 24 | 1 | 22 | 3 | 250 | t | 1 | 2 | 0 | 1 | MCI | ||||
| 25 | 1 | 36 | 2 | 2230 | 1 | 0 | 2 | 0 | 1 | 0 | 0 | VIM | ||
| 26 | 1 | 37 | 6 | 3375 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | VIM | ||
| 27 | 1 | 37 | 6 | 2183 | 0 | 1 | 2 | 1 | 0 | 0 | 1 | VIM | ||
| 28 | 1 | 2030 | 0 | 1 | 2 | 1 | 0 | 0 | 1 | VIM | ||||
| 29 | 1 | 38 | 2 | 2335 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | VIM | ||
| 30 | 1 | 36 | 2 | 1930 | 0 | 1 | 6 | 3 | 0 | 2 | 3 | VIM | ||
| 31 | 1 | 36 | 2 | 1880 | 0 | 1 | Twin | VIM | ||||||
| 32 | 1 | 36 | 4 | 1999 | 0 | 1 | 2 | 1 | 0 | 0 | 1 | VIM | ||
| 33 | 1 | 30 | 540 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | VIM | |||
| 34 | 1 | 40 | 3831 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | VUE | |||
| 35 | 1 | 38 | 0 | 2775 | 0 | 0 | 3 | 2 | 0 | 0 | 2 | FIM | ||
| 36 | 1 | 32 | 1091 | 1 | 1 | 3 | 0 | 2 | MCI | |||||
| 37 | 1 | 34 | 2 | 0 | 0 | 4 | 2 | 1 | VIM | |||||
| 38 | 0 | 1 | 1 | X | MCI | |||||||||
| 39 | 0 | 13 | 1 | FIM | ||||||||||
| 40 | 0 | 37 | 3 | 2990 | 0 | 1 | Y | 2 | 1 | 0 | 0 | 1 | MCI focal | |
| 41 | 0 | 37 | 4 | 2241 | 0 | 1 | 2 | 1 | 0 | 0 | 1 | FIM | ||
| 42 | 0 | 37 | 2180 | 0 | 1 | 4 | 0 | 0 | 3 | 0 | VIM | |||
| 43 | 0 | 32 | 0 | 2140 | 0 | 0 | 2 | 0 | 0 | 1 | 0 | FIM | ||
| 44 | 0 | 35 | 1 | 2110 | 0 | 0 | Y | FIM | ||||||
| 45 | 0 | 35 | 5 | 1873 | 0 | 0 | 2 | 1 | 0 | 0 | 1 | VIM | ||
| 46 | 0 | 38 | 6 | 3271 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | VIM | ||
| 47 | 0 | 36 | 6 | 2470 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | FIM | ||
| 48 | 0 | 38 | 0 | 2680 | 0 | 0 | 2 | 0 | 0 | 1 | 0 | FIM | ||
| 49 | 0 | 38 | 4 | 3220 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | FIM | ||
| 50 | 0 | 36 | 2 | 2280 | 0 | 0 | x | x | x | x | x | VIM | ||
| 51 | 0 | 37 | 2626 | 0 | 0 | 3 | 1 | 1 | 0 | 1 | VIM | |||
| 52 | 0 | 37 | 2735 | 0 | 0 | 7 | 6 | 0 | 0 | 6 | FIM | |||
| 53 | 0 | 38 | 6 | 0 | 0 | 3 | x | x | 1 | 1 | VIM | |||
| 54 | 0 | 38 | 3 | 2840 | 0 | 0 | 3 | x | x | 1 | 1 | VIM | ||
| 55 | 0 | 37 | 2 | 2275 | 0 | 0 | 2 | x | x | 0 | 1 | FIM | ||
| 56 | 0 | 37 | 2693 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | FIM | |||
| 57 | 0 | 21 | 407 | 1 | 1 | 2 | 0 | 1 | VIM | |||||
| 58 | 0 | 32 | 1091 | 1 | 1 | 3 | 0 | 2 | MCI | |||||
| 59 | 0 | 30 | 973 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | FIM | |||
| 60 | 0 | 29 | t | 1 | 2 | 0 | 1 | VIM | ||||||
| 61 | 0 | 36 | 3760 | 1 | 0 | 4 | 0 | 0 | 1 | 2 | VIM | |||
| 62 | 0 | 29 | 5 | 1340 | 1 | 0 | 2 | 0 | 1 | VIM | ||||
| 63 | 0 | 38 | 2870 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | VIM | |||
| 64 | 0 | 31 | 1094 | 1 | 0 | 6 | 2 | 3 | VIM |
Note: c4d= original classification of c4d staining; GA= gestational age; b.w.= birth weight in grams; plac wt= placental weight in grams; SB = stillbirth (1 is positive, 0 is negative); SGA= small for gestational age (1 is positive, 0 is negative); recurrence: letters (W-Z) represent an arbitrary designation linking recurrent cases; GTPAL= gravida, term, preterm, abortion, living (GTPAL data on recurrence was included only on the most recent pregnancy, in one dichorionic twin, the GTPAL: data was included on only one twin); POC= products of conception; histology MCI=massive chronic intervillositis, FIM = few intervillous monocytes and VIM= villitis with intervillous monocytes. Excepted as noted for GTPAL, empty cells are because not all patient data was available.
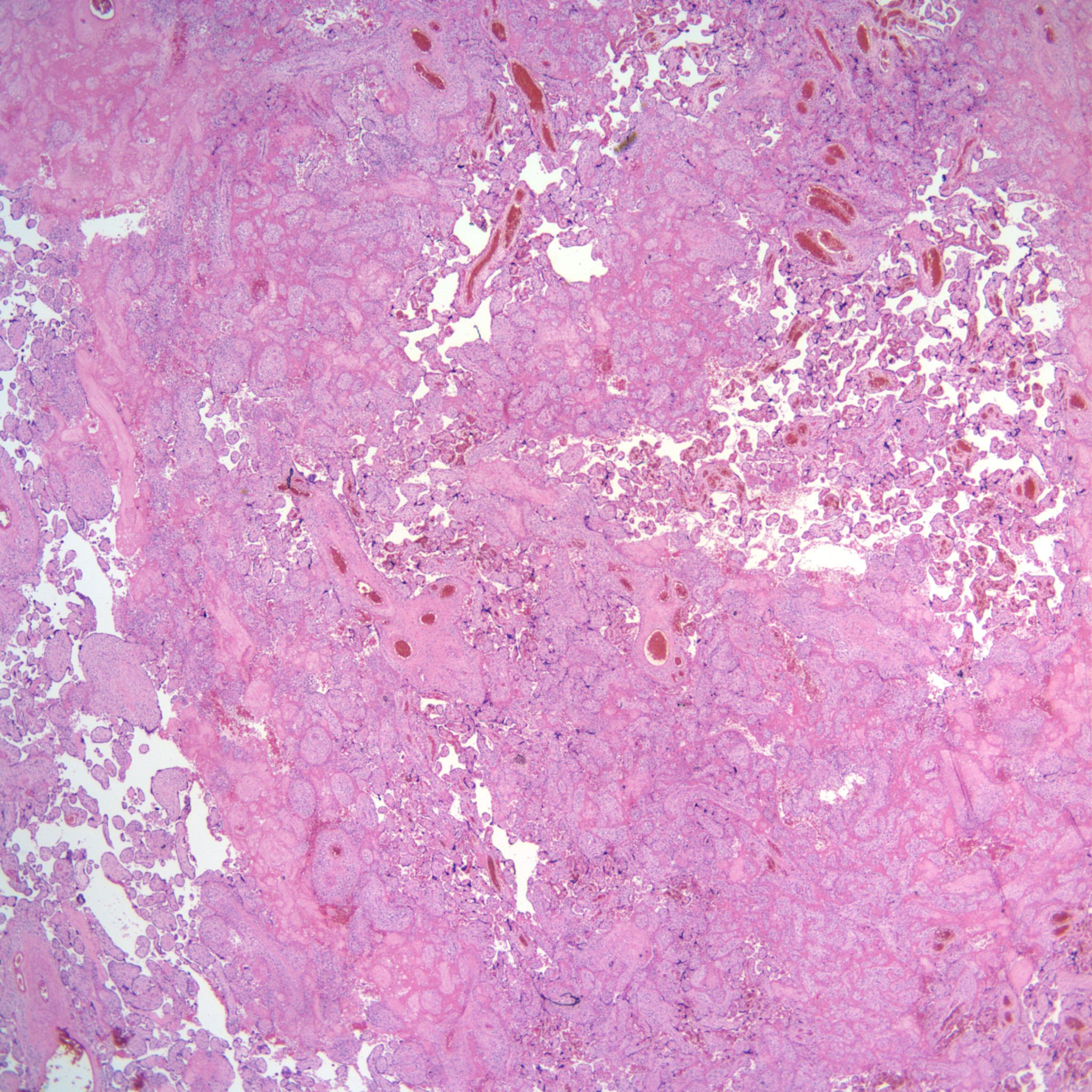
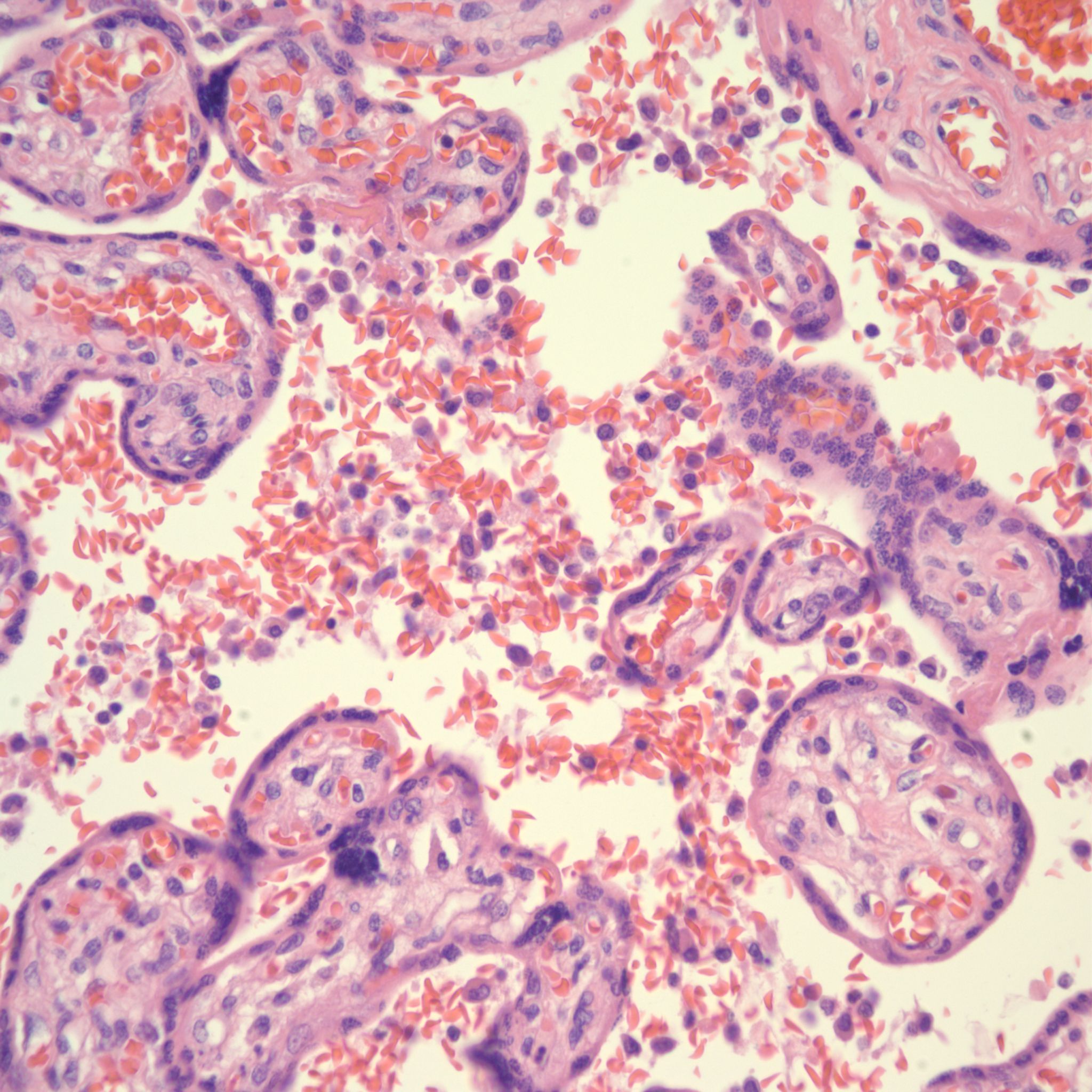
Figures for CHIV
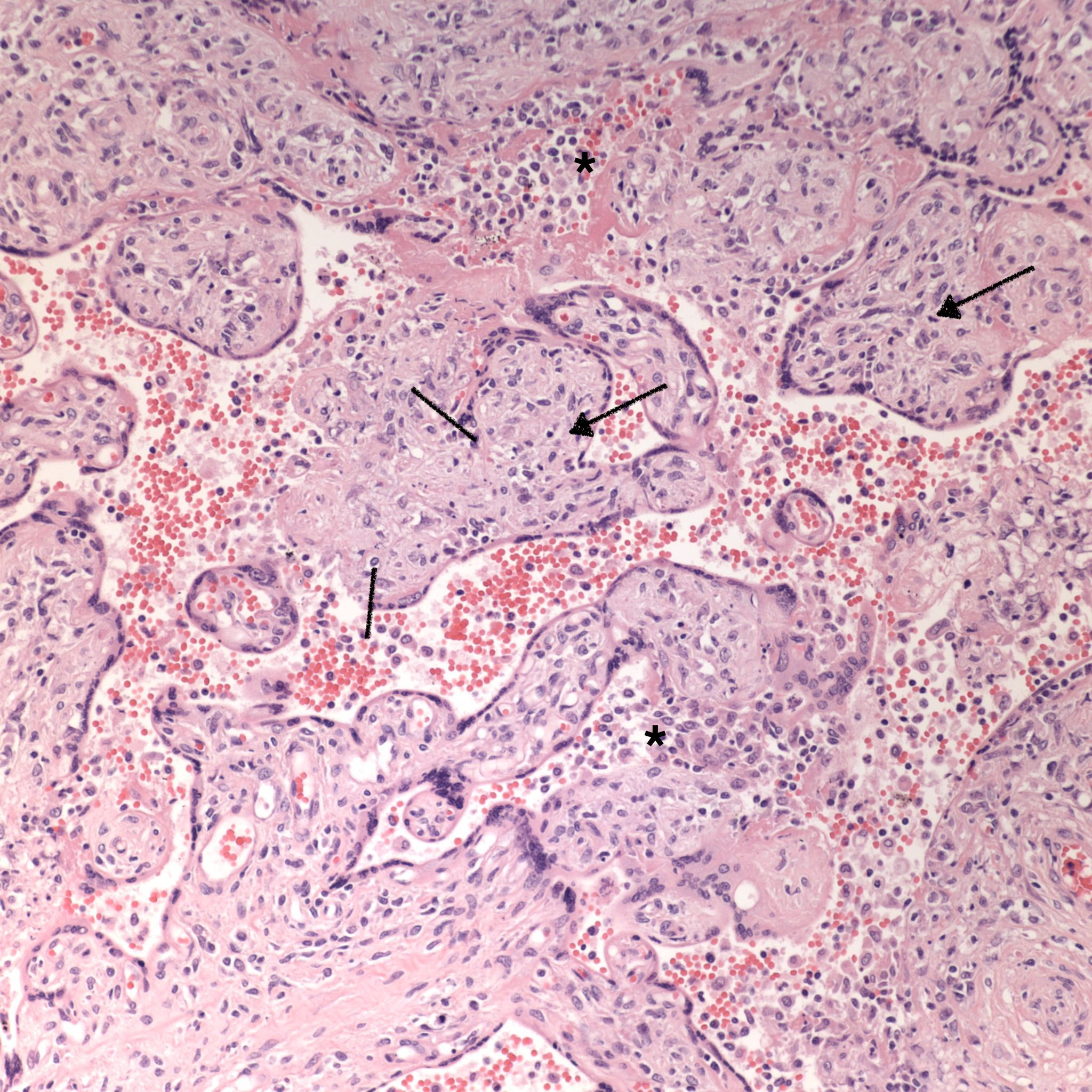
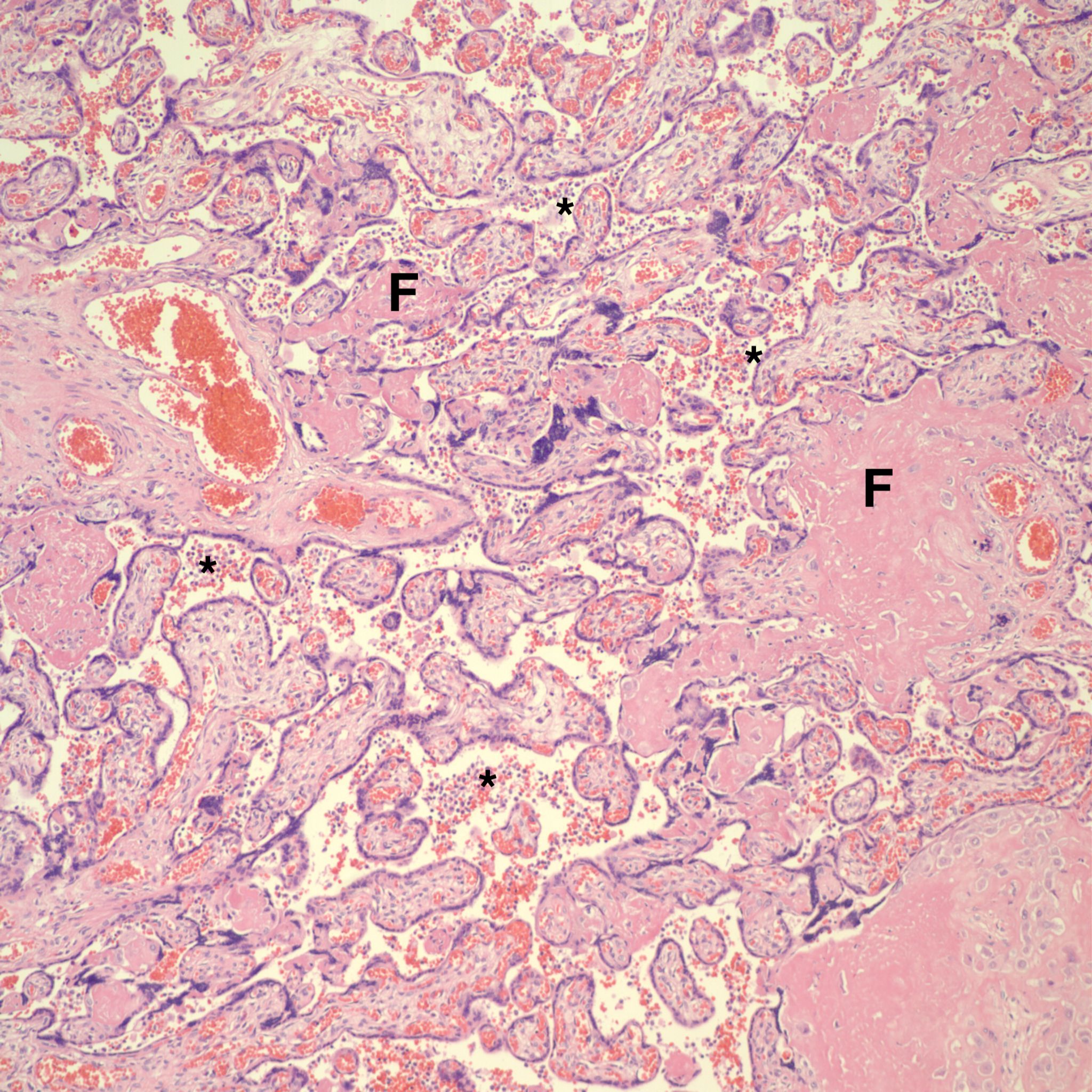
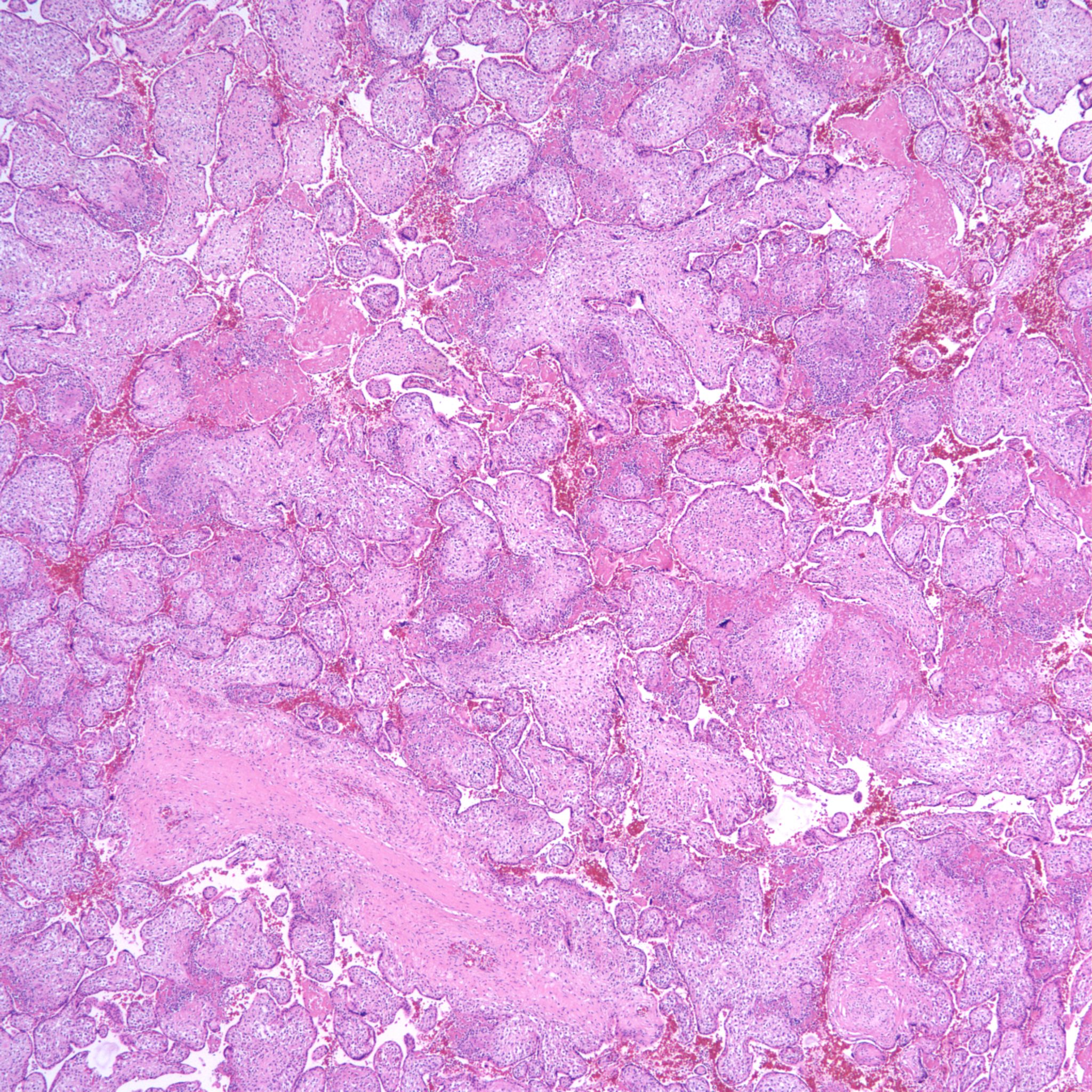
High Grade (massive) CHIV
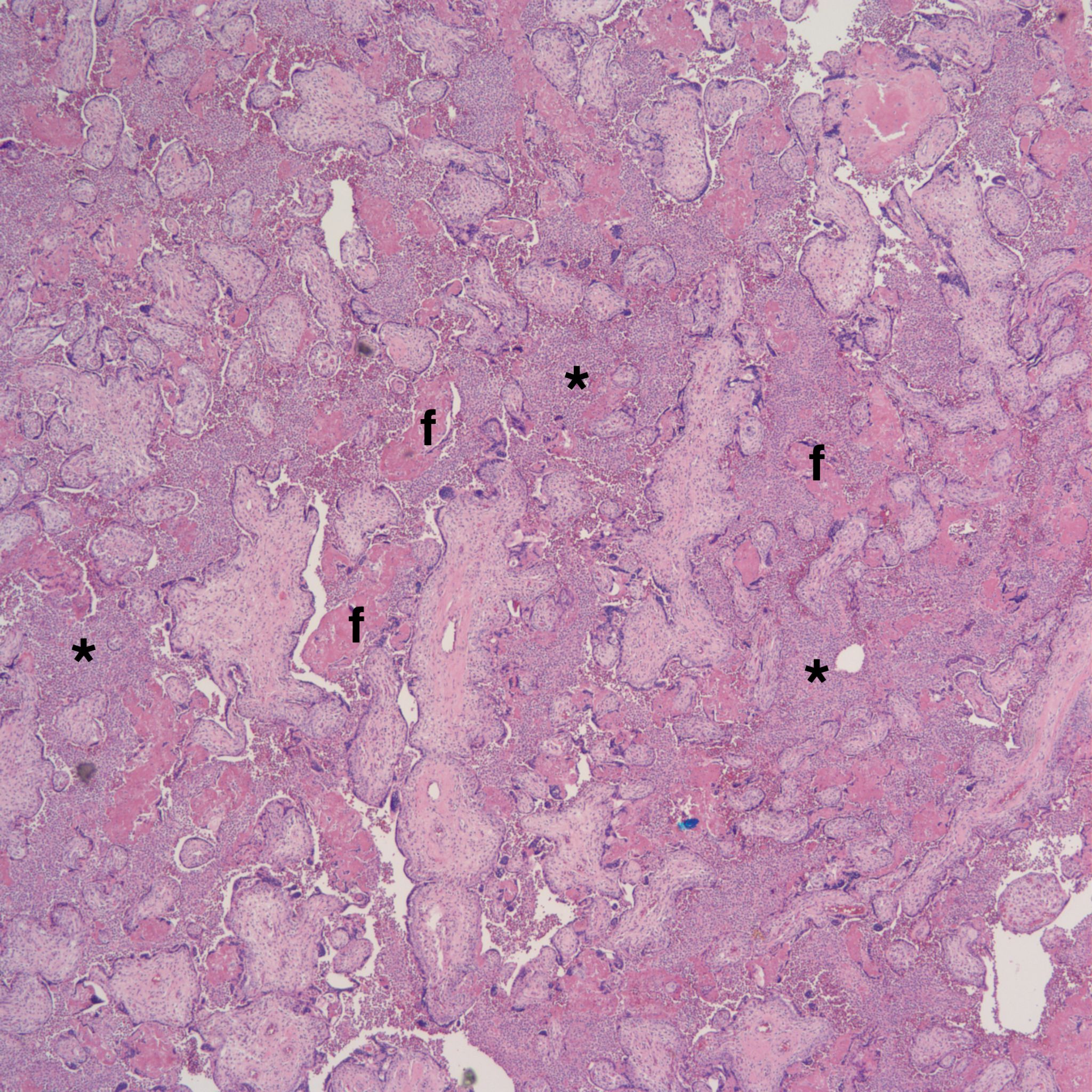


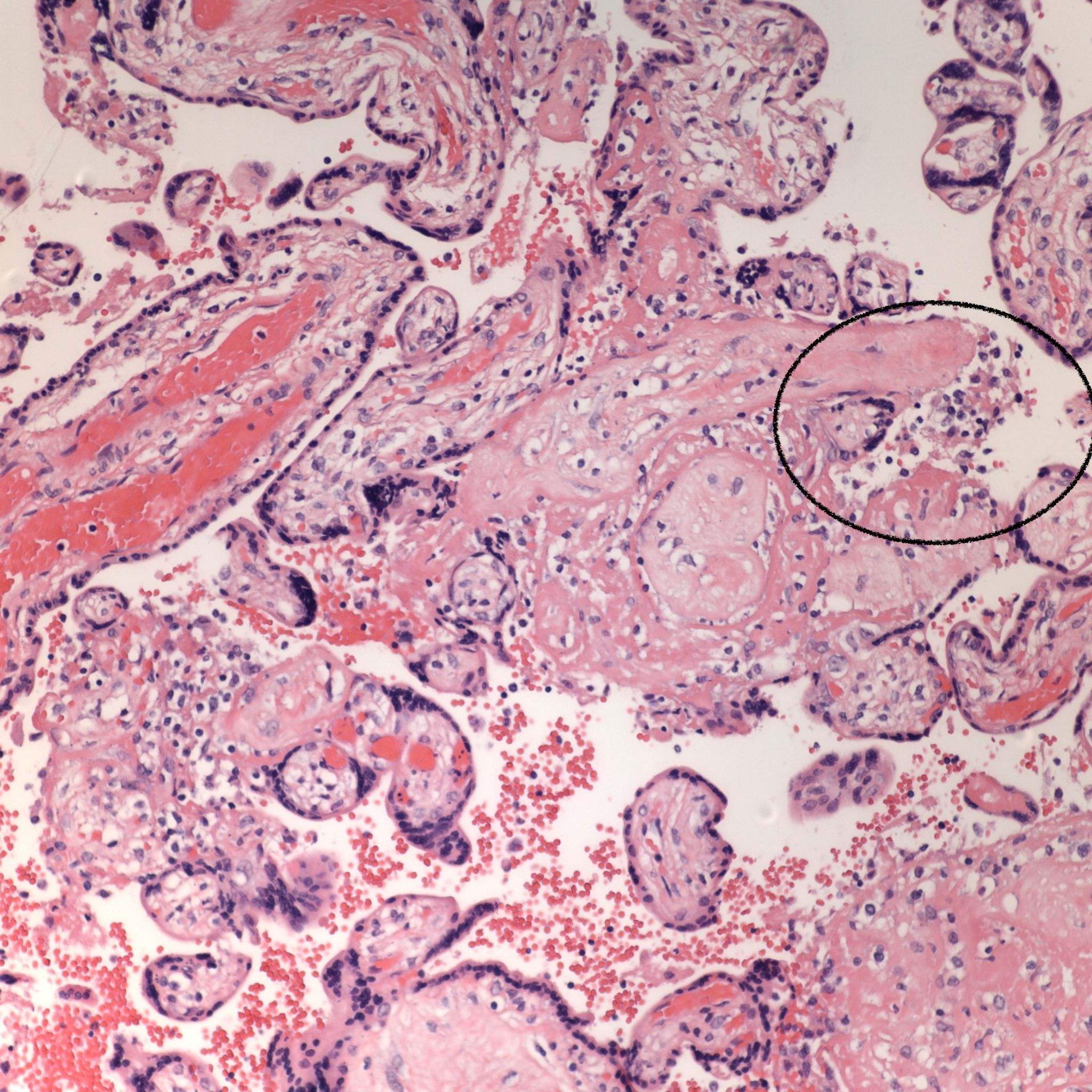
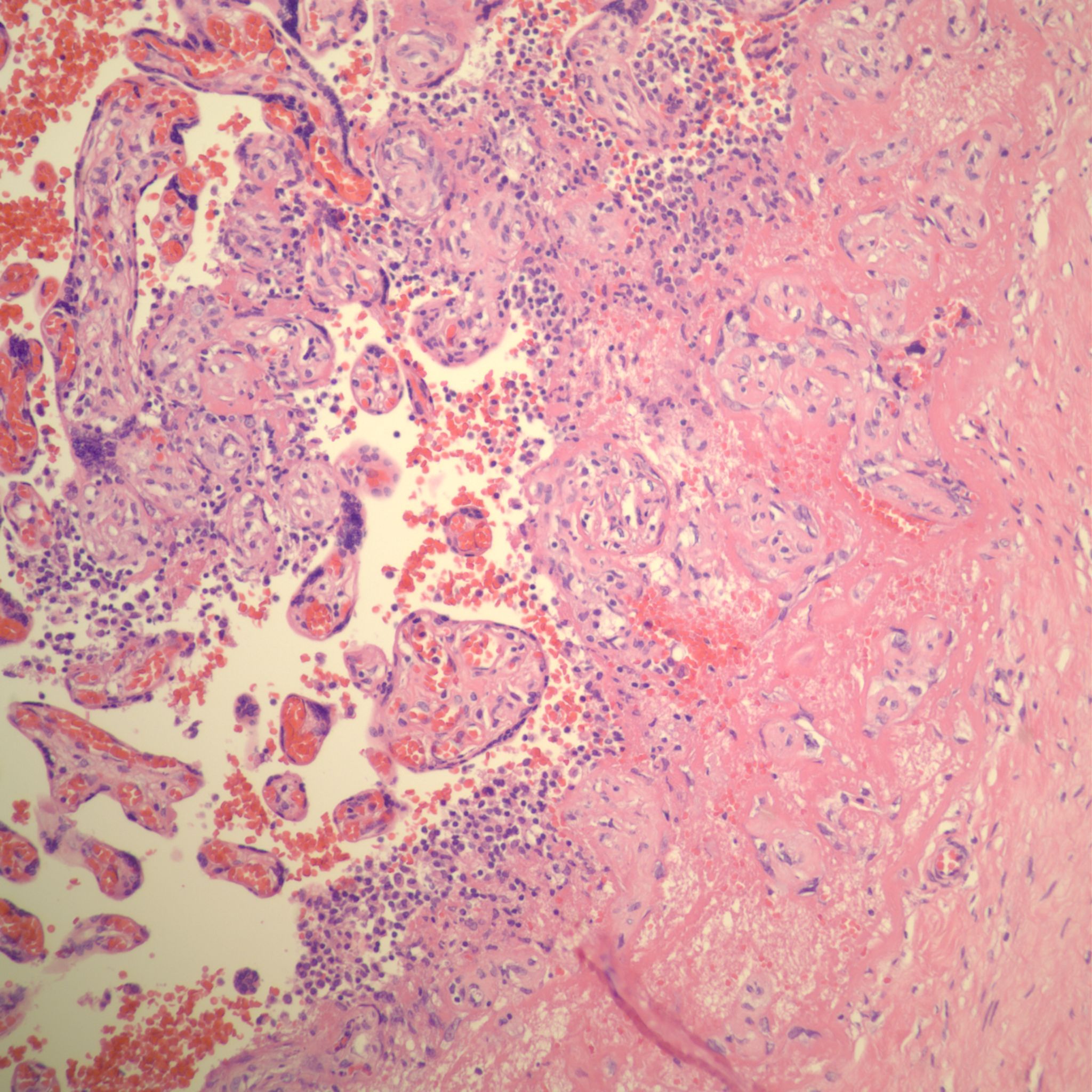
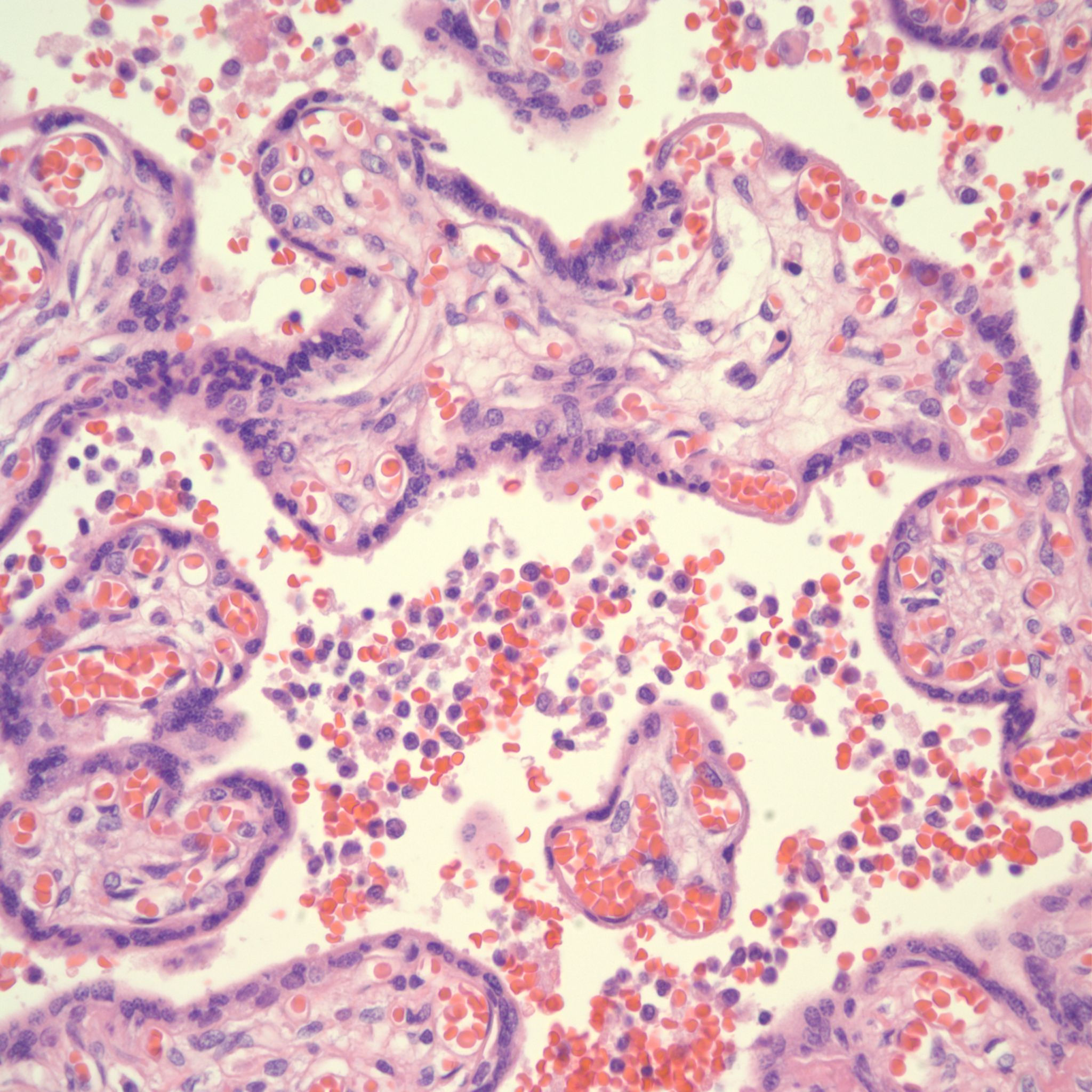
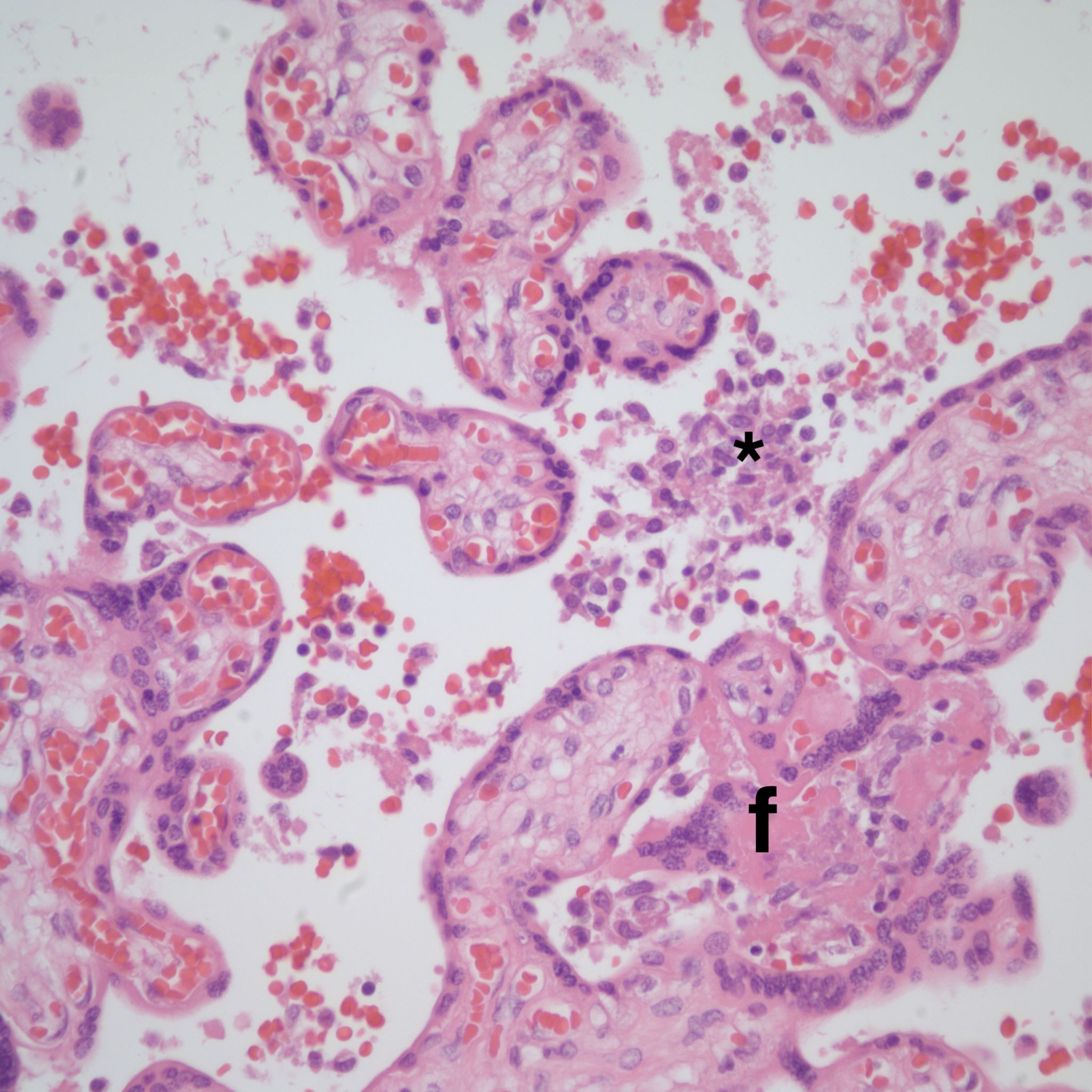
Low Grade CHIV (5-50% of the intervillous space occupied by monocytes)


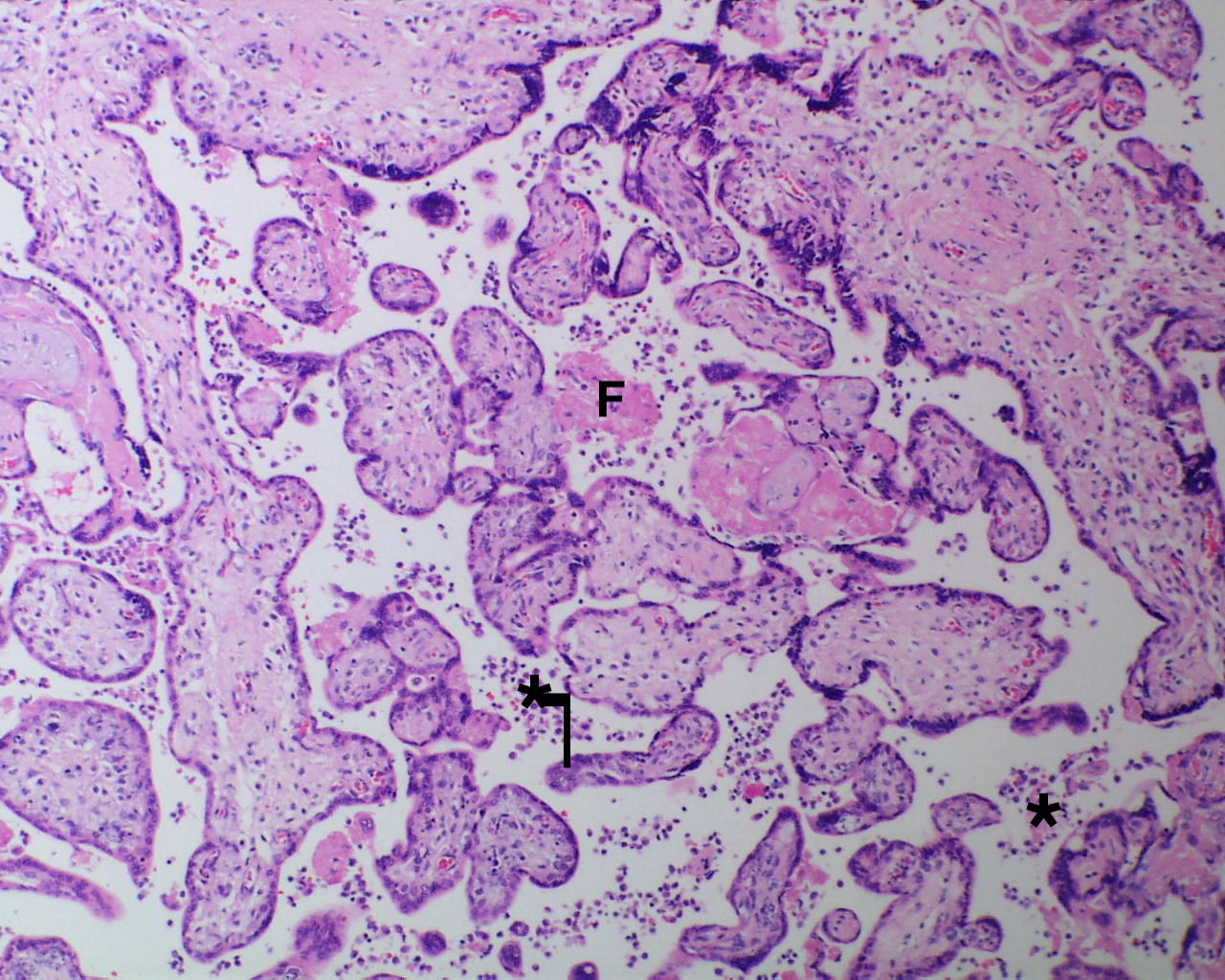
There is a focus of intervillous fibrinoid with no definite cytotrophoblast that is not re-covered with syncytium suggestive of recent syncytial injury (F). (10x, H&E)



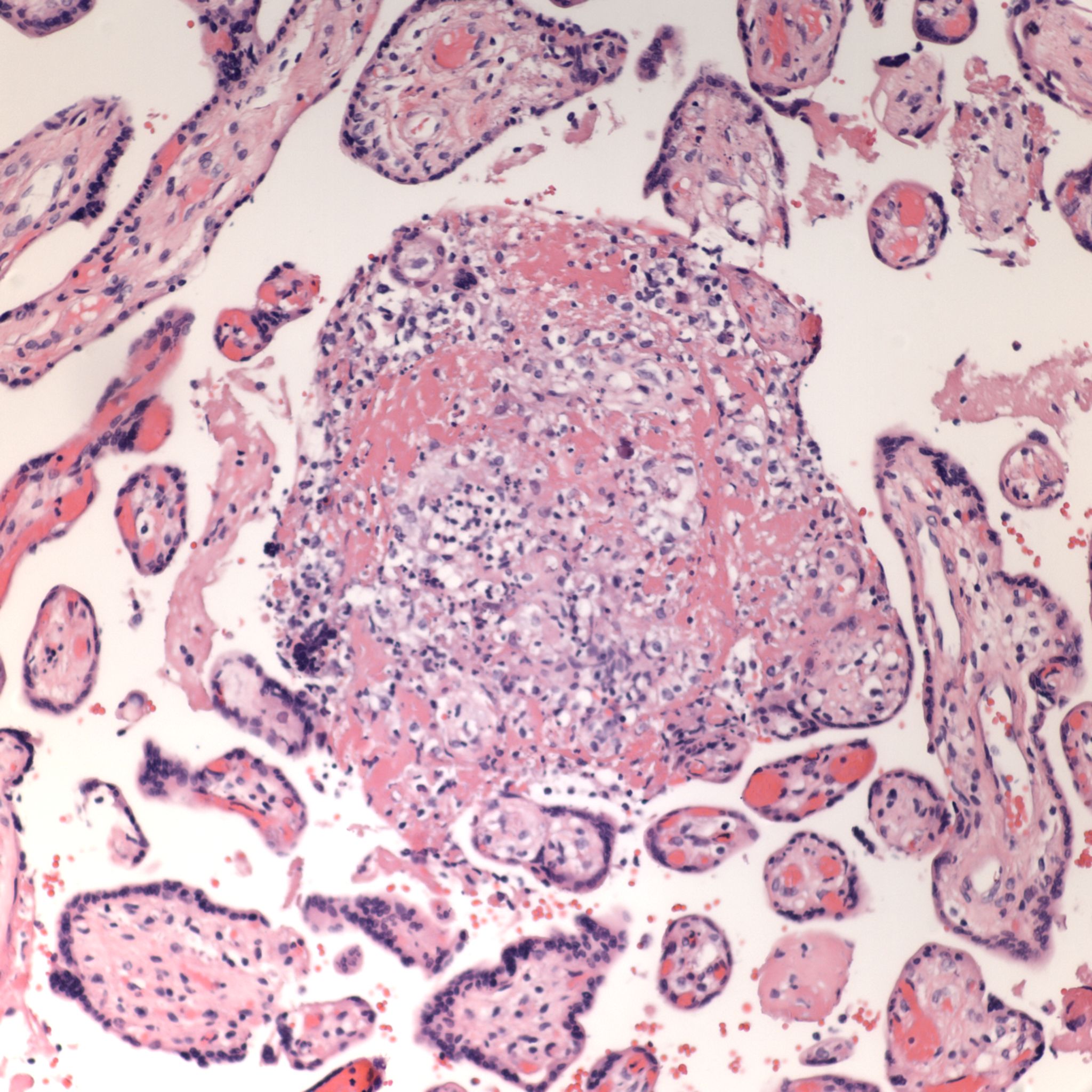
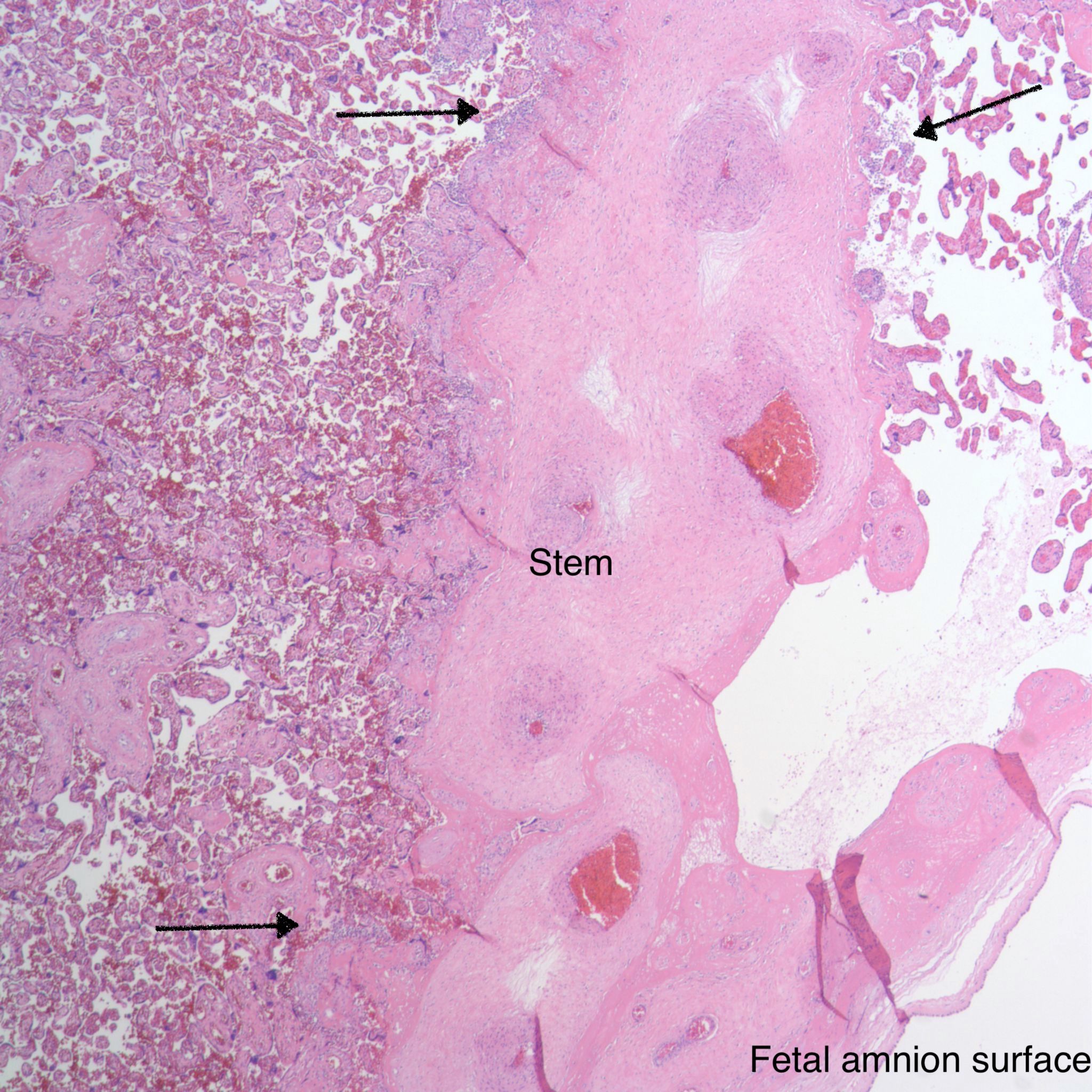
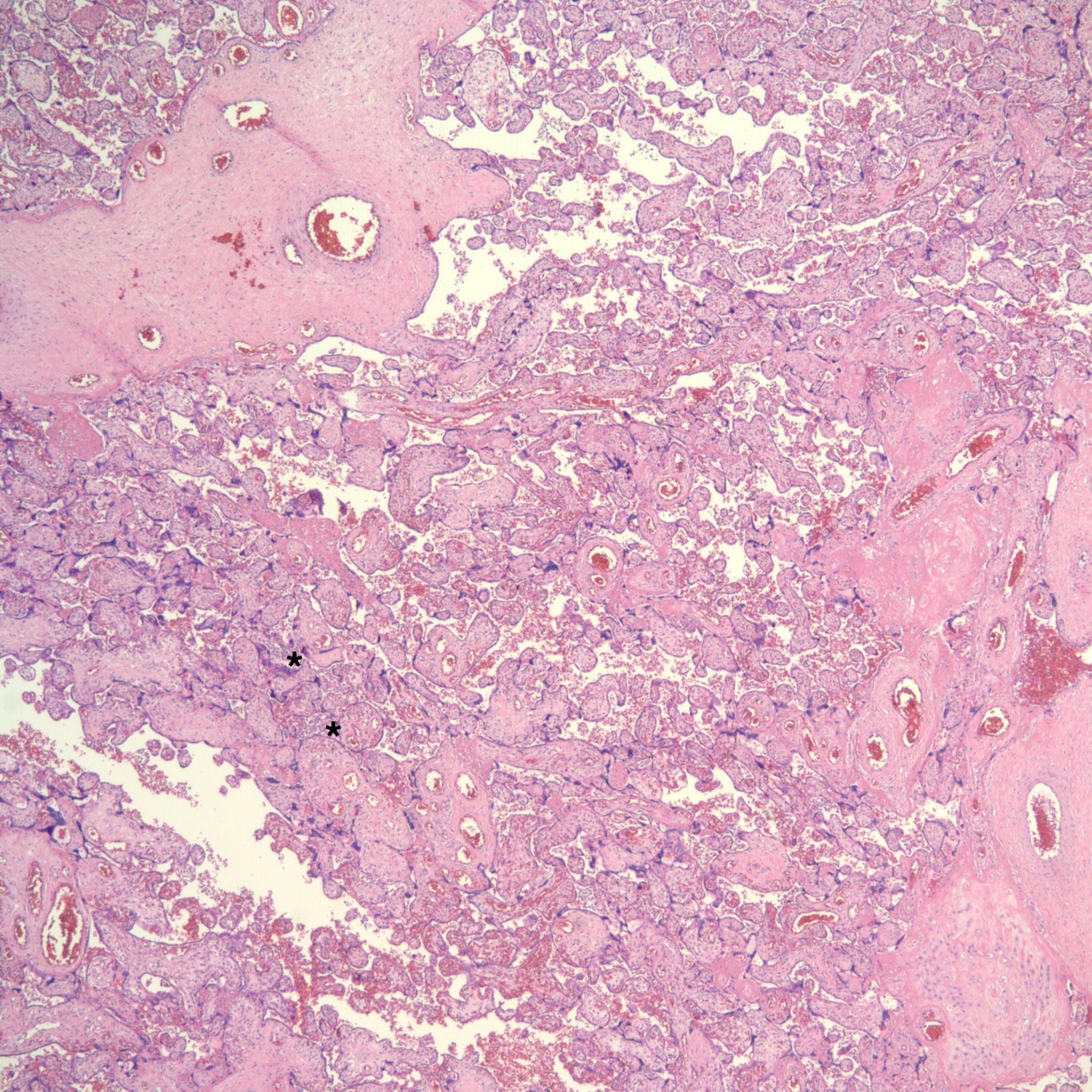
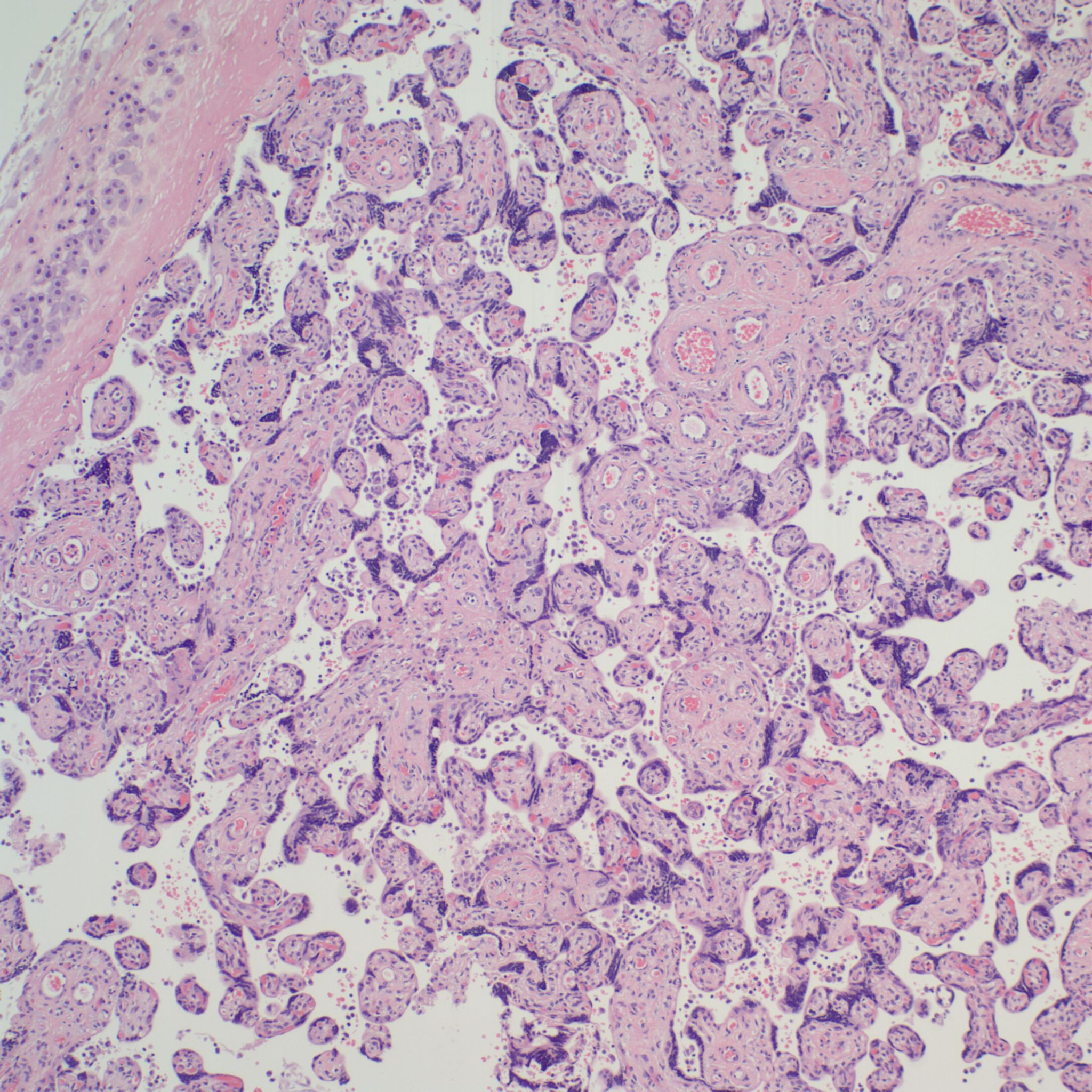
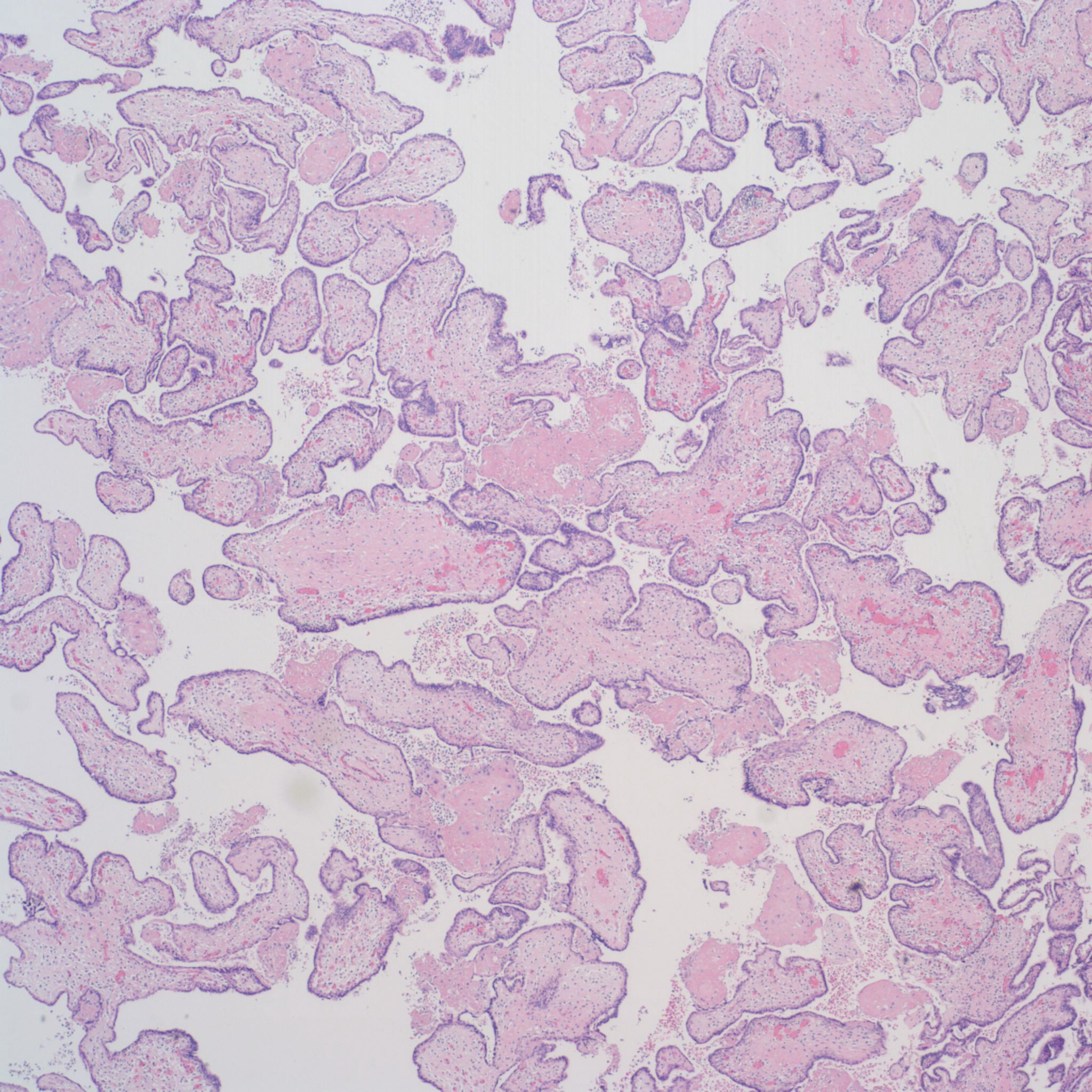
CHIV with prominent perivillous fibrinoid deposition



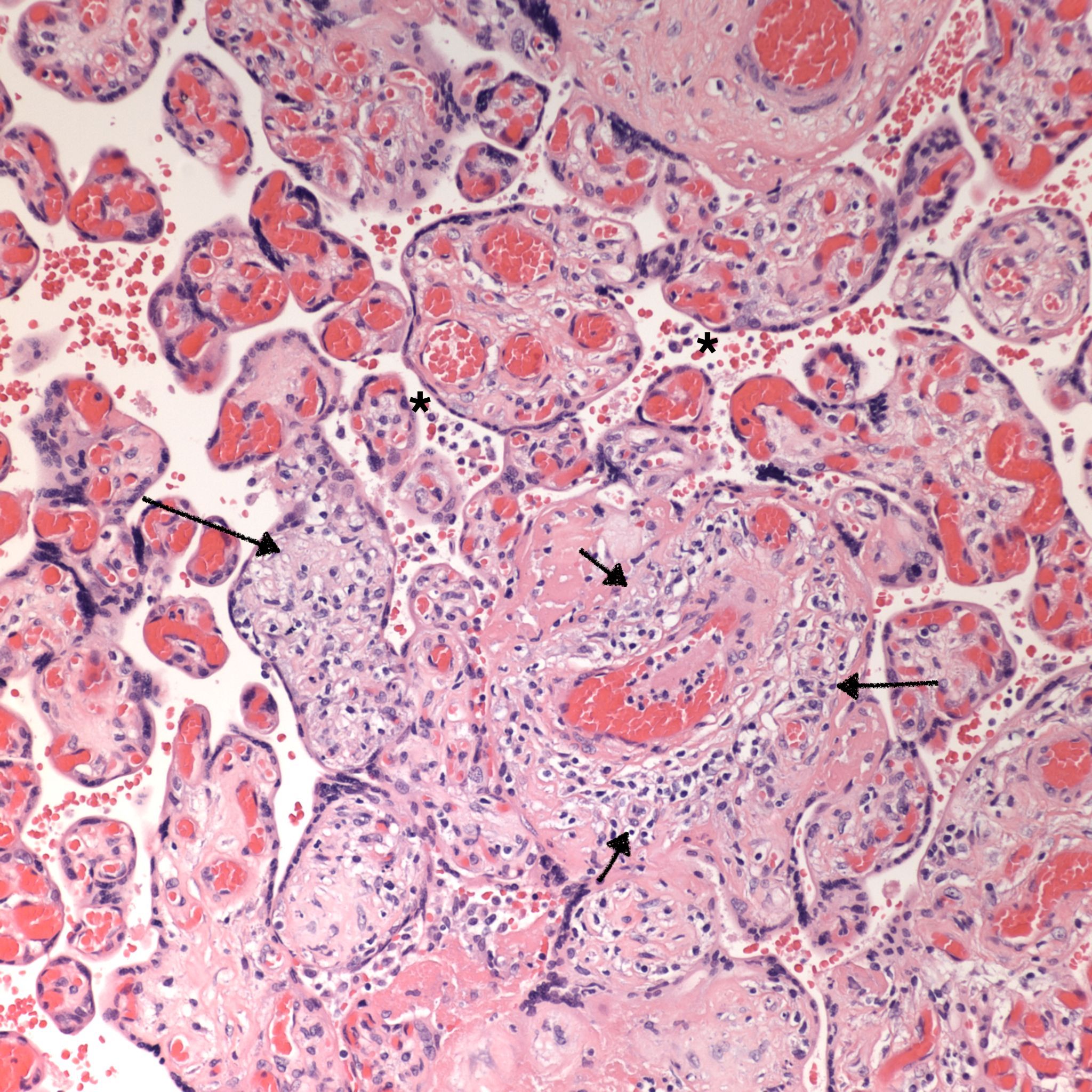
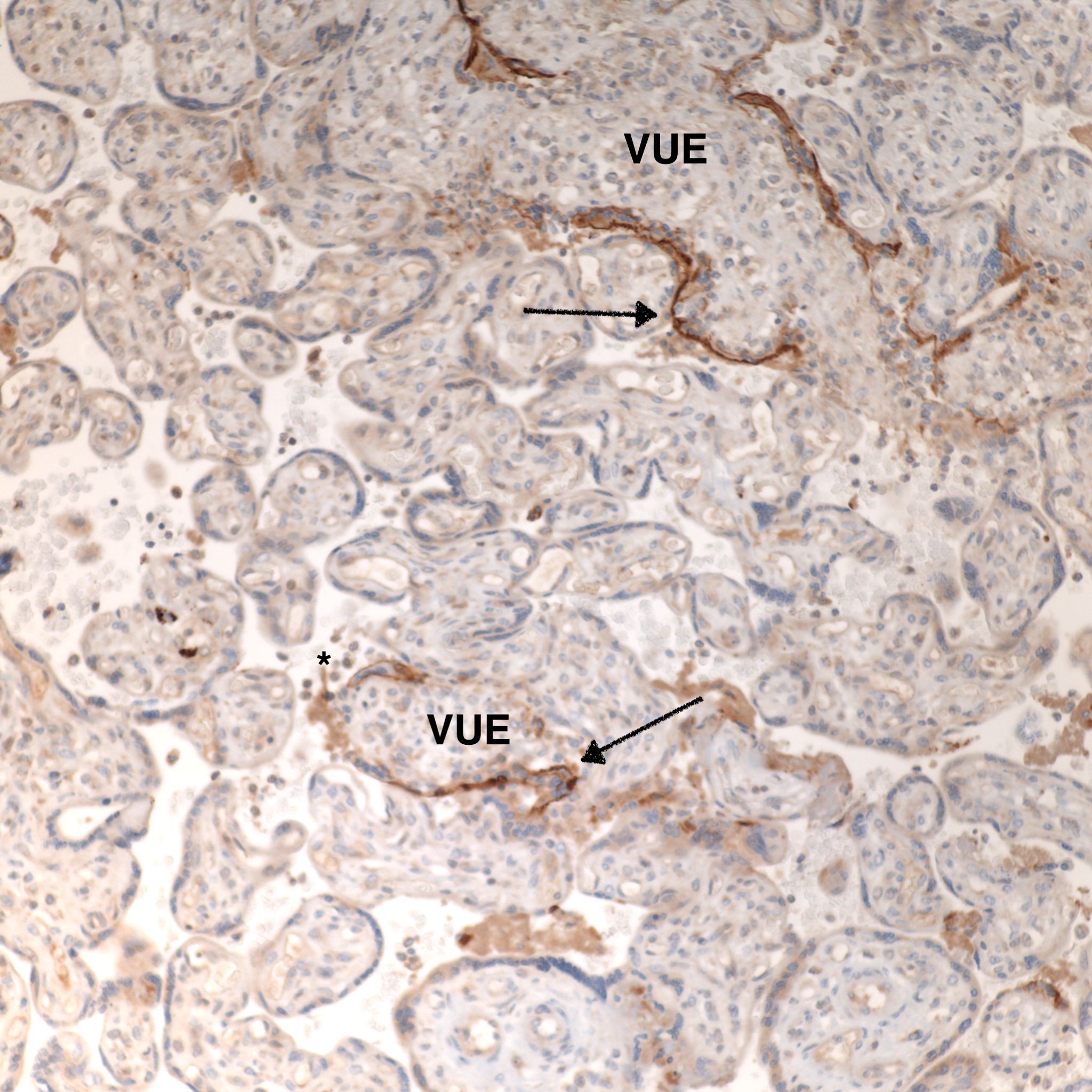
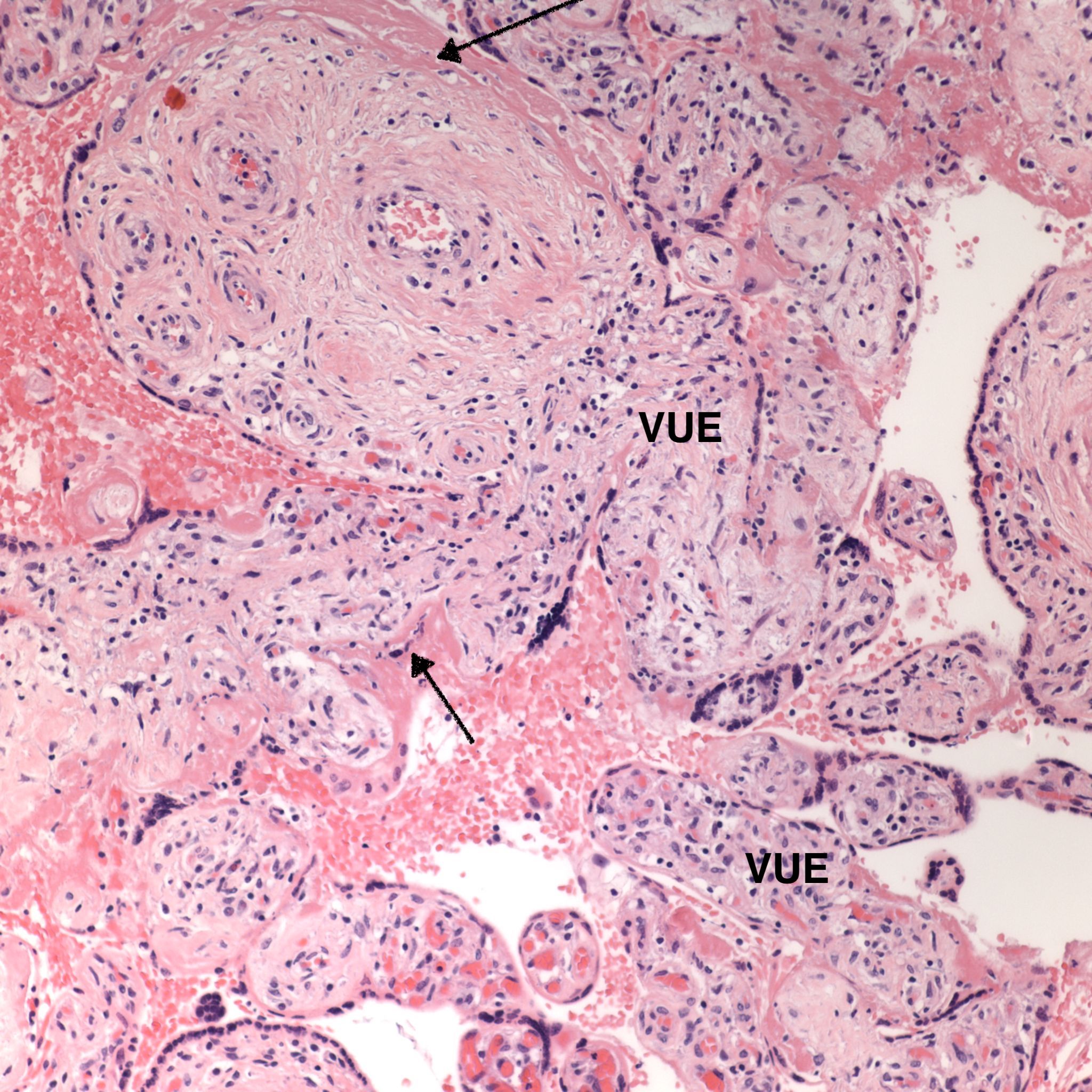
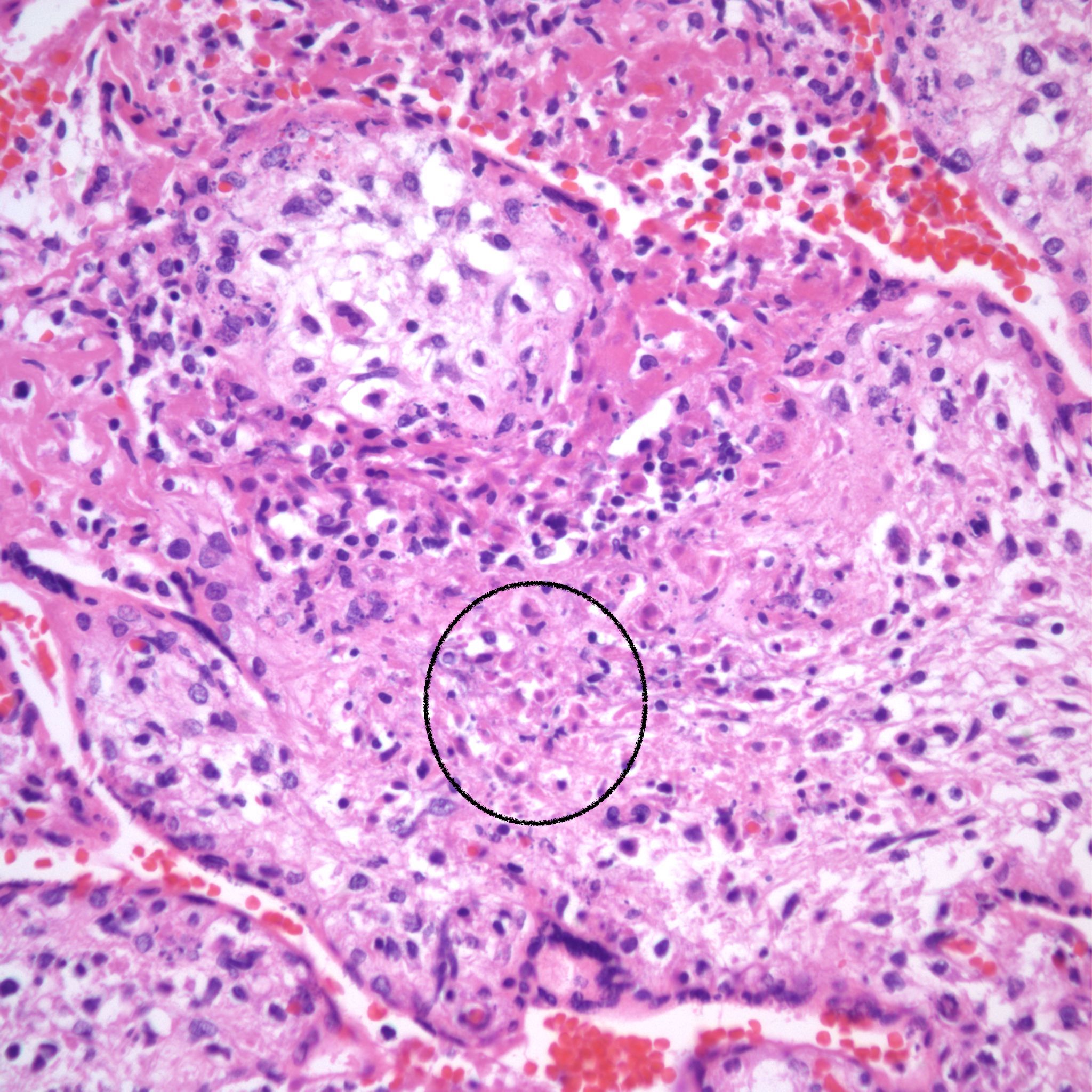
CHIV associated with Villitis of Uknown Etiology (VUE)
This pattern could be due to a primary cause of VUE with incidental chemotaxis of monocytes, two pathogenetically interrelated processes, or an incidental focus of VUE in a predominant CIIV disease. Currently, describing the extent of each process and its colocalization or lack of may prove useful until a better way to classify the co-existing lesions can be developed. One study has shown that there is a dichotomy between cases with c4d staining and those without c4d staining18.


Figures for differential diagnosis
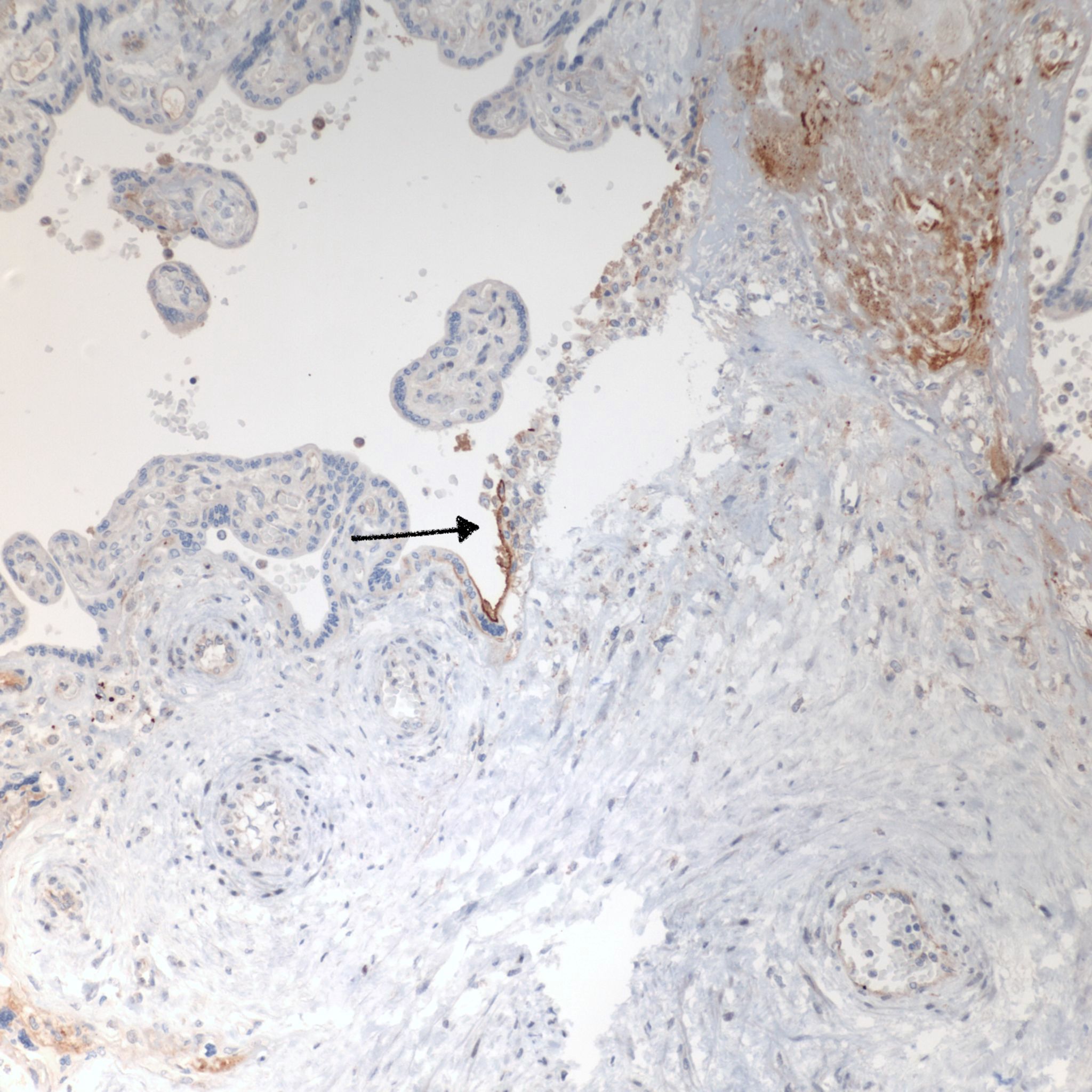
Focal Intervillous monocytes
1. Focal CHIV: One study found an unanticipated case with focal monocyte accumulation associated with focal c4d staining18. This finding perhaps merits a separate subclass designation as it contradicts the underlying hypothesis of the study that a circulating antibody is responsible for variable complement fixation along the surface of the villi. The marked focal lesion suggests that there is a change in just those villi, either a focal epigenetic/genetic change during development or a focal acquired change from the intervillous environment such as an infection. The complement fixation could still be initiated by a circulating antibody, or it could be initiated by a different complement fixing pathway.



2. Few Intervillous Monocytes
In otherwise normal placentas and pregnancies there may be small clusters of monocytes in the intervillous space, but these may not be evidence of CHIV etiology. The consensus criteria is less than 5% of the intervillous space, but this can be difficult to estimate since the monocytes are often focal, and the intervillous space includes many empty areas elsewhere on the slide. Still unproven, villous immunostaining with c4d may help identify the monocytes as having the same pathogenesis as CHIV. While not investigated, the finding of a subpopulation of MAC387 positive monocytes is a feature of CHIV that might indicate CHIV in cases with less than the diagnostic criteria of monocytes10.







3. Infectious Diseases with intervillous monocytes
a. Malaria
b. Cytomegalovirus (CMV)
c. Toxoplasma

Pathogenesis:
1. Direct evidence of Immune injury in intervillositis: The accumulation of monocytes in the intervillous space is the dominate evidence of an immune origin of intervillositis. The accumulation is likely due to both a chemotactic response and increase in either a cell adhesion molecular on the monocyte surfaces or possibly a secondary ligand that is linking monocyte surface molecules. One piece of evidence of an immunologic injury is the staining of the microvillous surface of syncytiotrophoblast by c4d, a stable complement product used routinely in pathology laboratories in identify antibody-mediated rejection in biopsies of transplanted organs. T-cells have been identified as a minority population in intervillostitis, but a regulatory role cannot be excluded. There is evidence in one study of in vitro T-cell activation.
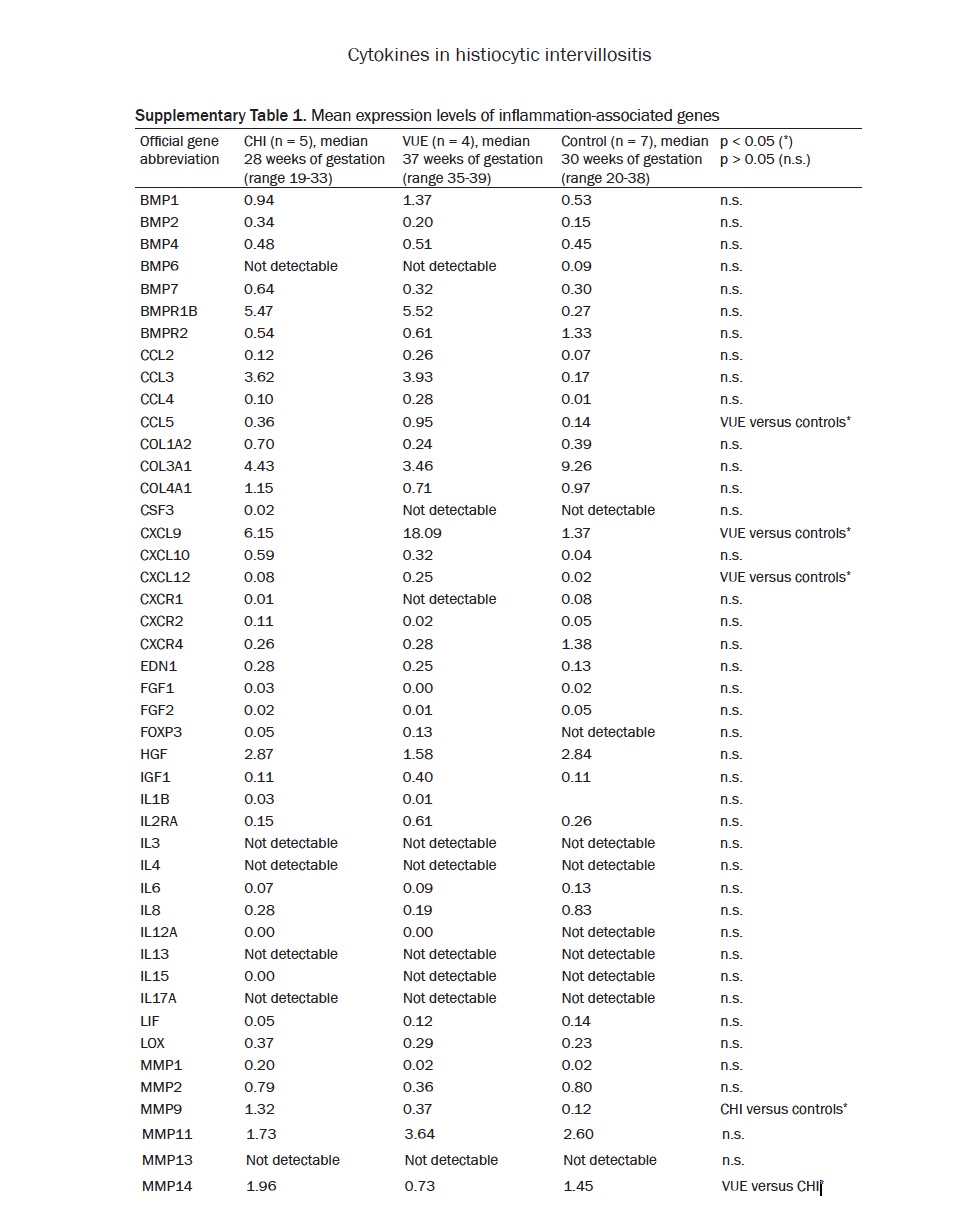
a) A study by Freitag et. al. compared 5 cases of CHI to VUE and controls by extracting RNA from paraffin tissue blocks using a large PCR array for expression of cytokine and angiogenesis genes19. The only significantly elevated gene expression in CHI compared to controls was for matrix metallopeptidase 9 and transforming growth factor beta receptor 1. These differences in means appeared to be due to 2 outliers with the other 3 cases having low values similar to controls. The samples would have included villi as well as monocytes. This study is more important as a negative study. The summary of tested genes is seen in these 2 tables:

2. The role of autoimmunity in some cases: Many reports have noted an association with various autoimmune diseases. Patients with a “tendency” to form autoantibodies, classically in systemic lupus erythematosus (SLE), may form antibodies to a variety of antigens that could include those expressed on the microvillous surface. These antibodies would do no harm until such antigens were expressed on the placenta. This same tendency could be an explanation for increased anti-HLA antibodies in some cases. The villous surface has Histocompatibility antigens, but not allogenic antigens. If the surface of the synctytiotrophoblast even though partially paternal in origin must not routinely have antigens that elicit an immune rejection.
a) The hypothesis could be tested with maternal serum in intervillositis, concentrating and labelling her antibodies with fluorescent dyes and the applying them to frozen sections of her placenta and a series of controls. It may be necessary to first wash the villous surface of antibodies already bound to the surface, and the then to block Fc receptors on the surface of the villi. Maternal fluorescent labelled antibodies could also be used against purified antigens that are known to be present on the microvillous surface.
3. The role of allo-immunization to paternal antigens: The high recurrence rate of intervillositis in some mothers suggests by analogy with Rh allo-sensitization and anti Pla1 platelet antigen allo-sensitization, the possibility that there is an antigen on the microvillous surface that is allogenic, with a much less frequent allele in the population. If so, the severity of the disease suggests that the allele is highly expressed, and likely vital as well. The mother would then have the rare antigen, and the father the common antigen. With the same father, if the paternal antigen was heterozygous, there would be on average a 50% recurrence rate, if homozygous, then the recurrence rate would be 100%, always assuming the same father. The mother would be homozygous for the rare allele. In Rh disease, because the fetal blood is not in direct contact with the maternal blood, sensitization is usually not symptomatic in the first pregnancy and likely occurs late in pregnancy with exposure to small leaks of fetal blood. With a microvillous antigen exposure would occur when the antigen became expressed on the trophoblast surface.
a) This hypothesis could be tested for similarly to that described above for antibodies. In addition, in case reports, it would be important to note if the father remained the same (not always easy to prove, but at least remarriages could be collected ) and if the first pregnancy was less effected on average than the later pregnancies.
4. Secondary aborters and lymphocyte-trophoblast cross-reactive antigens: These concepts were proposed in a series of papers by Faulk and McIntyre at the Center for Transplant and Reproductive Immunology. They started by examining the patient population who had one successful pregnancy, but all subsequent pregnancies ended in fetal loss. They reasoned this might be the result of sensitization to paternal alloantigens in the first pregnancy. Then by looking at mixed lymphocyte culture of maternal and paternal white cells from secondary aborters, they discovered that some maternal lymphocytes responded to paternal lymphocytes. This led to the theory that the maternal lymphocytes were responding to antigens on the surface of the paternal lymphocytes that were the same epitopes as those on the syncytiotrophoblast. They identified transferrin receptors as a likely candidate for the alloantigens. The concept was new but makes sense. If some antigens are expressed exclusively on syncytiotrophoblast microvilli, they might not be available for the development of immune tolerance, that is recognized as self, by fetus. A logical solution is that these necessary but otherwise hidden antigens would be expressed on lymphocytes, and hence recognized as self, even if not expressed in the fetal (as opposed to placental) tissues. It is possible that the monocyte adhesion is related to the cross-reactive antigen, suggesting that the antigen expression is dense on monocytes, but may be rare on lymphocytes.
a) As noted, it is possible that in intervillositis that the first pregnancy may be severely affected unlike the cases of secondary aborters. However, if indeed intervillositis is due to lymphocyte cross reactive antigens, the testing for alloantiboides can be done on maternal and paternal lymphocytes, which can be done without a sample of the mother’s placenta, before or after the pregnancy. There is one paper that reports mixed lymphocyte culture activation in intervillositis but they attribured the reaction of HLA antibodies. More research of this type needs to be done, as such a cross-reactive antigen could be the basis for simplified testing for intervillositis by identify maternal antibodies in vitro to the paternal antigen.
5. Perivillous fibrinoid and intervillositis: Many studies mention the association of intervillositis with syncytiotrophoblast necrosis and pervillous fibrinoid deposition. The syncytiotrophoblast provides features of an endothelium with plasminogen activators. If the villous surface is injured and the underlying stroma is exposed, this is a trigger for the coagulation cascade in similar other circumstances such as in endothelial injury in blood vessels. Pervillous fibrin formation could follow, but unlike intravascular thrombi, in the placenta, the process demonstrates a mix of the underlying cytotrophoblast cells and their presumed secretions of annexins, etc. These are the same substances normally secreted at cytotrophoblast interfaces with maternal tissue. This mixture is usually referred to as fibrinoid. Such syncytiotrophoblast injury and hence perivillous fibrinoid deposition can occur in other conditions. In the case, of intervillositis, as evidenced by cd4 staining, one mechanism of syncytiotrophblast injury is likely activation of the complement cascade on the microvillous surface. The increase in perivillous fibrinoid due to intervillositis needs to be measured against the expected background deposition which can vary by gestation or diseases such as preeclampsia, as well as by normal variation by location within anatomic regions of the placenta such as below the fetal surface or along maternal septa.
6. Villitis of unknown etiology (VUE) and intervillosits. Our current understanding of VUE is that the pattern of inflammation is due to a vasocentric attack by maternal T cells on villous capillaries. Since the interior of the villus does express HLA alloantigens, such a rejection response is plausible. How these lymphocytes breech the syncytiotrophoblastic barrier is not clear. Theoretically, gaps due to injury in the syncytiotrophoblast could allow entry. A perivillous fibrinoid response which is not only fibrin, but the normal substances secreted by cytotrophoblast at maternal interfaces, such as fetal fibronectin and annexins, may normally be a sufficient barrier to prevent maternal T lymphocyte entry into the villous. However if syncytial necrosis in intervillositis was rapid and extensive, a breach for T lymphocytes maybe created that could account for the association of the two lesions. In this case, the villitis would be secondary to the intervillositis. The finding of c4d staining in some cases of the mixed lesion supports this hypothesis. In other cases, the two lesions may be independent. VUE is common placental finding likely for multiple different etiologies. There may be value to noting if the intervillositis and villitis are in the same or contiguous areas, and positive c4d staining may also demonstrate a causal connection. VUE with intervillositis may like fibrinoid be a measure of severity and extent of the syncytial injury.
7. Intrauterine growth restriction in intervillosits: All three lesions of trophoblastic injury, namely intervillositis, extensive VUE, and extensive perivillous fibrinoid deposition, are associated with fetal growth restriction. They represent a different model of fetal growth restriction different from models of decreased utero-placental perfusion, cytotoxic or infectious agents, or genetic/epigentic abnormality including trisomies. The syncytiotrophoblast is the site of intense energy/oxygen dependent active transfer of nutrients to the fetus. Loss of active microvillous transport function is the most likely common denominator of this mechanism of fetal growth restriction. There is some evidence that it is the most severe.
a) This hypothesis could be investigated in growth restricted infants with intervillositis compared to similarly growth restricted infants from other mechanisms by measuring in the nursery their relative storage of transported substances such as iron or calcium. (Massive perivillous fibrinoid deposition is associated with hyopmineralized bones, but this is complicated by the binding of calcium to fibrinoid substances such fibronectin and annexins.
8. Focal intense intervillositis with c4d staining: Intervillositis is usually widely distributed, although not necessarily evenly, in the intervillous space. A very focal lesion surrounded by normal parenchyma suggests either a focal expression of an allotype, or possibly a localized infection that like some infectious villitis may have a low focal penetrance. The significance of this finding is unknown.
9. Monocyte clustering: The adhesion of monocytes to each other in the intervillous space and presumably binding at least focally to the syncytiotrophoblast has been studies in malaria. In Chronic intervillositis, there could be antibody binding of an antigen common to the surface of both monocytes and syncytiotrophoblast. While the monocytes often appear to be free floating on the microscope slides, the flow of blood in the intervillous space makes it unlikely that they are not anchored. However, being in the flow begs the question do they interfere in the flow. Does this blocked flow contribute to the fetal growth restriction. Since small monocyte clusters can be present without c4d staining, and without meeting the criteria for chronic intervillositis, do they have other pathologic or physiologic significance in pregnancy.
Literature Review
1. Meta-analysis: A comprehensive meta-analysis was published by Bos et.al. in 20181. They did not consider case reports of less than 3 cases, nor publications limited to abstracts of presentations. As within any such analysis they had to account for differences in definitions and inclusion and exclusion criteria. One difference they could not account for was the preponderance of retrospective pathology-initiated reports which would in many cases have had an ascertainment bias such as the inclusion of more abnormal patient selection for example for examination of the placenta for growth restriction in preeclampsia.
Case Series:

a) Boyd and Redline, 200010: This is a retrospective chart review of 21 mothers with a diagnosis of CHV with review of one representative slide for diagnosis from 45 specimens of which 31 had CHIV, thus 10 more pregnancies in the 21 mothers had CHIV. The diagnosis of inclusion was accumulation of intervillous monocytes. VUE was a basis for exclusion. There were a total of 97 pregnancies in these 21 mothers (only 1 mother was G1) but presumably slides were not available on more than 45.
(1) Special Stains: on 10 selected slides. Intervillous cells were 90% CD68+, and 30-40% of these were MAC387 +. (This protein for calprotectin or calcium binding protein MRP14 is a marker of activation of immature macrophages).
(2) Recurrence: 8 patients had ≥ 3 pregnancy losses, 5 primary (without living children) and 3 secondary with one living child (In table says following one living child). Text states 5 of 10 with more than 1 pregnancy had 2 or more spontaneous abortions.
(3) Fetal deaths: There were 50 spontaneous abortions, and 12 elective termination of pregnancies, and clearly not all had histologic specimens. In table 1, 61 cases of 1st (n=52) and 2nd (N=7) trimester cases, 36 were examined, and 26 had CHIV (N=23, N=5). There was a total of 25 infants from 20 to ≥ 37 weeks with 22 living children, but not clear if the losses were previable second trimester deliveries.
(4) IUGR: In the second trimester 1 of 3 CHIV cases had IUGR, and 4 of 5 in the third trimester based on the clinical determination in the record.
(5) Autoimmune: 3 of the CHIV mothers had an autoimmune disease not otherwise specified. (They also noted that 5 had asthma and 3 had drug allergies, but no control numbers). Since cases were in order in 2 tables, the history of these patients was that one had 7 spontaneous ab and no living children, one had 2 spontaneous ab and one living child, and the third had 1 spontaneous ab and 2 elective terminations.
(6) Treatment: One patient received prednisone in 2 subsequent pregnancy and had 2 living infants, and had less intense CHIV microscopically.
(7) Incidence: The study was based on searching for pathology cases with CHIV, and not incidence. In the discussion, the estimates for one of the two hospitals in the study, 9.6/1000 spontaneous abortions, and 0.6/1000 third trimester abortions. There are two biases using specimens. More placentas are sent from abnormal pregnancies which would increase the number of cases with IUGR, and “products of conception” in are more often submitted in mothers with more than one loss.
(8) Comment: The strengths of this study is the clarity of inclusions and exclusions, the consensus diagnosis from two experienced pathologists, the relatively large number of cases, and the wide array of immunostaining of the inflammatory cells. The idea would be a prospective study of an unbiased population of specimens, but with a rare disease that cannot be detected without the pathology specimen, this would be a very difficult study. Information that might be useful would have been: 1) the specific 3 autoimmune diseases. 2) to have identified if a living child had preceded the fetal losses in all of the cases, and 3) instead of excluding VUE with CHIV, keeping it as a separate category.
b) Koby et.al (2018) is a review of 35 women with pregnancy greater than 18 weeks of gestation, identified by pathologic diagnosis, not excluding VUE if small in amount20. The study relied on review of placental slides, fetal ultrasound usually at 22 weeks and last ultrasound prior to delivery or intrauterine fetal death, and on chart review of clinical history and of maternal serum screening for aneuploidy and for alkaline phosphatase. Only 2 of 27 multiparas had one normal pregnancy. See spreadsheet
(1) Comment: Does not include cases identified before 18 weeks, thus not comparable to many studies. Has no complications in 9 subsequent pregnancies in cohort, and of 7 with pathology no recurrent CHIV. A reasonable question is whether these patients differe from populations identified in under 18 week pathology. Alk phos was not a meaningful screening test in this group
c) Marchaudon et. al.(2011) is a retrospective review of 69 cases of CHIV from 50 patients found pathologically including spontaneous abortion, but excluded cases with other co-histopathology21. CHIV and PVF were graded as severe-confluent, moderate-heterogenous, and mild-few. Methods state slides stained with CD68. This study included for IUGR (≤3rd percentile) SB gest age detected 22±6 and at birth 28±4, IUGR LB 27±4 and 34±3. The study grouped birth into <32, 32-37, >37 weeks, For SB 12/4/2 for LB 4/9/8. The information for recurrence is complicated.
(1) Comment: This paper had more details than easily fit in a spread sheet, but like all studies found increased spontaneous abortion, stillbirth, and recurrence of both in multiparous women. They found less pervillous fibrinoid in fetal death unlike earlier studies which may be due to earlier gestation. They classified both monocytes and fibrinoid into three grades, but this still needs to be confirmed in other studies. They found Alk Phos correlated with IUGR.
d) Nowak et.al. (2016) is a retrospective study of all spontaneous abortion and complicated placentas that had either CHIV, VUE or a combined lesion22. There were 3 cases below 22 weeks and 21 above, in a population of 42,000 deliveries, yielding approximately .6% of deliveries. It was clear if the spontaneous abortions were included in the delivery total. The VUE and mixed lesions while differing in some measures from the CHIV, did not significantly differ from each other. They classified grades of the lesions, and divided IUGR into 3 percentile groups as well as recorded severity of antenatal doppler studies.
e) Ongaro et.al. is a histologic study of pathologist agreement on grading of 20 cases using both the percentage of both monocytes and fibrinoid associated with monocytes23. The cases were obtained retrospectively at a Children’s hospital, but consisted of 15 first and 5 second trimester fetal losses. While moderate kappa scores were obtained, with fibrinoid evaluation being a source of disagreement. They point out that the 5% level needed for diagnosis is not based on proven clinical significance, and this is a problem for all classifications.
f) Revaux et. al. (2015) Identified 12 women with an adverse pregnancy outcome and CHIV with 18 CHIV placentas in 4,292 that were examined24. These patients were referred for examination for autoimmune disease. The authors presented the clinical information as 12 index pregnancies, 16 prior pregnancies without pathologic diagnosis, and 10 subsequent pregnancies. Seven of the patients were diagnosed with an auto-immune syndrome, 4 with anti-phospholipid syndrome, 1 Sjogren syndrome, 1 pernicious anemia, and one celiac disease. There were no thrombophilias, and no significant other differences between CHIV with and without autoimmune disease. Treatment regimens all included low dose aspirin either alone or with prednisone, low molecular weight heparin, or hydroxychloroquine
a) Simula et.al. (2020) is a retrospective study of 47 patients (56 specimens) based on pathological diagnosis. The population prevalence was not estimated, but they found that the prevalence of CHIV in the first trimester specimens was significantly more than in the second and third trimesters (.38% v .09%) with a specimen base of 29,899 for 27,968 patients. These numbers would be biased by the criteria for submitting the specimens to pathology. They broke specimens down at follows: (11 of 1,906 autopsies > 20 weeks (.58%), 6 of 2591 autopsies < 20 weeks (.23%), 3 of 15,587 placentas(.02%), 36 of 29,445 products of conception (.38%.) The autopsy prevalence is high. They compared intervillositis cases with CHIV by Bos criteria, with those that failed to meet the criteria, and report only a significant increase in loss with those who met the criteria, with the numbers of autoimmune disease (4/39 v 3/33) and recurrent fetal losses (27/46 v 17/38) similar in both groups. They also found no difference between low or high grade lesions. There data was complicated by the use of varied treatment regimes. The rates of prior and subsequent pregnancy loss were similar in N=121 pregnancies from 38 women and 36 from 21 women. They found IUGR often severe based on abdominal circumference 7/15 infants greater than 20 weeks of gestation but not significantly altered by grade. They comment that while they had high recurrence, they often did not have pathological diagnosis to confirm recurrence of CHIV and that the varied treatment regimes precluded comparison. They did not find high prevalence of autoimmune or alkaline phosphatase.
Overall comments: (This section could have different comments by different editors. My goal is to try to synthesize the evidence from the literature and my experience with cases with twofold purpose, 1) to identify an approach for future studies and 2) to be able to write a reasonable Final Diagnosis comment. This is meant to my personal opinion, and comments and contradictions are welcome. )
1. Prevalence: The prevalence in term of total births is likely below 0.5% but is likely higher is cases of non-chromosomal first and second fetal loss. Institutional estimates of prevalence that used pathological diagnosis were biased by the indicators for pathological examination. If specimens were sent because of recurrent first or second trimester loss, or from complicated pregnancies, the prevalence would appear increased.
a) Research: Planning studies for a needed significance level would have to be based on an estimate of gestation at detection. Resources would be saved by using higher risk population such as early gestational onset of growth restriction, a history of recurrent fetal loss, or a history of CHIV in a prior pregnancy.
b) Diagnostic report: A comment can state that the diagnosis of CHIV is associated with an elevated risk of fetal loss (and as discussed below), fetal growth restriction and recurrence in subsequent pregnancies.
2. Recurrence: Cases series have demonstrated an increased rate of recurrence of the lesion in subsequent pregnancies. Determining the rate of recurrence is complicated by the lack of pathological diagnoses on pregnancies prior to the index case, and by lack of knowledge of all subsequent pregnancies. Some women have had normal pregnancies after the diagnosis, while others have had persistent fetal loss up to 9 in a row.
a) Diagnosis: The note should state that the risk of recurrence in subsequent pregnancy is high.
b) Research: The ordering of lesions by occurrence in a mother’s obstetrical history would help understand when the pathology began (for example primary v secondary recurrent fetal loss pattern) and for similar reasons if possible a change in the identity of the father (although if this is an anti-antigen disease, the rare genotype would be maternal)
3. Gestational age at onset: CHIV has been identified in all gestational trimesters.
a) Diagnosis: The pathologist needed to be aware that the lesion may occur at any gestation.
b) Research: There is a need to understand the factors underlyng the different gestational ages at onset. What factors result in survival to a later gestation? Do mothers with recurrence, present with fetal death or growth restriction at a similar gestation?
4. Criterion for diagnosis: The consensus criterion for the pathological lesion are inflammatory cell clusters in more than 5% of the intervillous space with 80% or more of the cells being of monocyte lineage. Most authors exclude infectious cases of intervillositis. The grading of the lesion generally was based on intervals of the percentage of the intervillous space filled with monocytes. The consensus was a scheme proposed by Roti et. al. which is basically dividing cases by greater or lesser than 50% of the intervillous space. The outcome to the fetus could be unrelated to the number of monocytes, as their accumulation could be an epiphenomenon, and for example, the underlying fetal growth restriction could be due to microvillous damage on the syncytium. Some studies have have found that even the greater than 5% criterion may not change the risks of growth restriction or death for the fetus.
a) Diagnosis: The Final Diagnosis should be based on the consensus criteria, currently those of Bos. The use of the Roti severity grading has not been proven useful, but at the discretion of the pathologist could be added. There are two important steps prior to committing to the diagnosis 1) The mother should not have a monocytic leukemia and 2) the blood smear (or blood on the placenta slide) should not demonstrate malaria. Clinical or pathologic evidence of blood borne infection in the infant should not be present. In these later conditions the diagnosis becomes that of the infection. If the monocytes are < 5% of the intervillous space, a comment can be added that there are intervillous monocytes that fall below the consensus diagnosis for CHIF. The significance of this finding is unknown.
b) Research: The Roti grading could be noted, but a less biased approach would be to include all cases with identified clusters of intervillous monocytes on screening and then count them in a specified area of parenchyma on the slide for a number of monocytes per placental area. If three samples of placenta are routinely chosen from non-marginal, non-lesion areas, and if the counting is a mid-centimeter square, the sample will not be truly random, but since the sampled areas with these restrictions are similar for all, then each case has a similar (and meaningful) area of the placenta has an equal chance of being selected, and therefore statistical variance should be valid. The numerical value could then be analysed as a receiver operator curve.
5. Perivillous fibrinoid: CHIV is often associated with an increase in perivillous fibrinoid. Determining the amount, if any, can be difficult. The placenta normally forms fibrinoid along intervillous surfaces that lose their trophoblastic surface such as beneath the fetal chorionic plate and along stem vessels, or along maternal septa, as well as in areas of ischemic injury such as the margins of old infarctions. There also is a baseline of perivillous fibrinoid along previously functional villi that appear to entrap a core or arise from a gap in the syncytial surface (not always in the same plane of section). At some point, the accumulation of perivillous fibrinoid from unknown mechanisms is associated by itself with the same complications as CHIV, namely fetal growth restriction, fetal death, and increased maternal risk of recurrence in subsequent pregnancies. One hypothesis is that perivillous fibrinoid is due to focal denudation of syncytiotrophoblast with preservation of cytotrophoblast that causes the expansion of the lesion, perivillous fibrinoid deposition. This pathogenesis could be a common pathway for more than one mechanism including a pathway the produces CHIV.
a) Diagnosis: The perivillous fibrinoid deposition given present knowledge should be evaluated independenlyt of CHIV by the pathologist’s usual criteria.
b) Research: One objective measure would be the volume of fibrinoid in the same areas in which monocytes are counted. A more difficult measure, but perhaps more meaningful measure of extent in the percentage of denuded syncytiotrophoblast. Automated methods rather than stereometry would make the process less burdensome, perhaps with different stains such as CD-68 and counterstained with PAS.
6. Villitis of unknown etiology (VUE): Authors have varied in whether to exclude or include CHIV with VUE, or some compromise. Some studies have suggested that the combined incidence of VUE and CHIV is greater than chance, although VUE is much more common, on the order of 6% of placentas. VUE has also been associated with an increased incidence of fetal growth restriction, fetal death, and maternal recurrence, but at much lower incidences and with more dependence on the extent of the lesion. The pathological collision of CHIV and VUE can vary from predominant CHIV with a few isolated villi with VUE to extensive VUE with some clusters of monocytes. VUE is caused by maternal T-cells that have entered the villus, where they are exposed to paternal HLA allogenetic antigens. Monocytes in the intervillous space are exposed only to non-allogenic HLA but to potentially allo-antigens from functional microvillous proteins. The interaction between these two pathological processes is unknown.
a) Diagnosis: The diagnosis of VUE should be included as a separate diagnosis treated as the pathologist normally provides a diagnosis of VUE.
b) Research: Until the pathogenetic relationship between the lesions is understood, VUE can be quantified as a percentage area in the three 1 cm areas sampled for CHIV. The usual description if VUE could be included for possible analysis as well. In these cases, a combination of T-cell and monocyte immunostaining as well as c4d would help elucidate the relationship of hypothetically cellular rejection (VUE) and antibody mediated rejection (CHIV). A potential substudy would be to classify the cells in the villi in male fetuses by those of maternal or fetal origin. Those in typical VUE are of maternal origin.
7. Acute inflammation: Some studies have excluded cases with chorioamnionitis, but there is no proven basis for such exclusion of a this common lesion of ascending infection. More difficult is the distinction histologically of monocyte clusters with neutrophils from acute intervillositis whether from ascending or blood borne infection, such as with Listeria micro-abscesses.
a) Diagnosis: Chorioamnionitis should be made by the usual diagnostic criteria. If neutrophils compose the cellular infiltration in the 20% of non-monocytic intervillous inflammation, microabscesses should be looked for including reexamination of the gross specimen then if absent, a comment might be appropriate that a separate acute intervillositis cannot be excluded although CHIV is present.
b) Research: As for diagnosis, acute inflammation does not preclude the diagnosis of CHIV nor remove the need to look carefully for acute intervillous lesions.
8. Focal lesions: Some authors have classified the degree of homogeneity versus heterogeneity of the density of monocyte clusters. Even more puzzling is the finding of an isolated patch of that in a very restricted area meets the criterion of CHIV. Given the limited sampling of the placenta, this finding may be an extreme of a heterogenous lesion, rather than a true solitary lesion. However, a focal lesion could have a different pathogenesis than more diffuse lesions.
a) Diagnosis: A comment can be made that there is focal lesion that meets in that area criteria of CHIV, but has no known significance.
b) Research: Heterogeneity of the density of intervillous monocytes to some extent can be measured by the range in the three counted samples. A separate category of focal CHIV would allow including or excluding the lesion as CHIV in analysis.
9. Intrauterine growth restriction (IUGR): The technical problem is determining growth restriction at all gestations, and which criteria to use. A clinical determination based on either a known conceptional day or on very early ultrasound, compared to fetal size/weight below a given percentile either by ultrasound or birthweight (or crown heel length) using norms for gestational age can be used to create a normalized basis for IUGR. If there are no clinical measurements nor a fetus to be examined as in some product of conception specimens, then growth restriction cannot be determined. In viable gestational age infants, usual criteria can be utilized.
a) Clinical: As noted above a comment of the association of CHIV with growth restriction is appropriate
b) Research: The basis of determination of gestational age, the earliest gestation of detection, the percentile of size/weight, and the birthweight or (crown rump) for gestation at birth may all be useful parameters to analyze especially for treatment evaluation.
10. Autoimmune disease: The association of CHIV to autoimmune disease has been suggested especially with antiphospholipid antibodies. This is a pathogenetically plausible but unproven association, as large enough series of CHIV cases compared to controls are still not available.
a) Diagnosis: The pathologist might comment that these is a possible association of CHIV with autoimmune disease in the mother.
b) Research: A clinical history of autoimmune disease can be recorded, and antiphospholipid antibodies measured. Serum can be retained to search for specific auto or allo-immune antibodies against placental or lymphocyte antigens.
11. Evidence of allo-immune antibodies: Given the high rate of recurrence and the evidence the evidence of monocyte activation in the intervillous space, as well as c4d deposition on the microvillous surface of the syncytiotrophoblast, an maternal antibody to a paternal antigen(s) is a plausible pathogenesis of the lesion.
a) Diagnosis: Without further evidence this hypothesis does not affect the pathologic diagnostic report
b) Research: Finding a specific maternal antibody or even a more specific pathologic pathogenesis would aid detection, diagnosis and treatment. If the pathway involves classical complement fixation, then maternal serum complement levels, and c4d red cell measures during and after the pregnancy may be diagnostic. Searching for a specific antibody can be performed on maternal serum, starting with a panel of frozen placenta sections from the mother’s and other placentas. The placental section can be blocked for Fc receptors, exposed to maternal serum and then detected with anti-human-IgG antibodies. More complex studies can be done if indicated and may include living lymphocyte/monocyte samples from the mother or father. Further study of the monocytes in the intervillous space might also provide insight into the pathogenesis.
Proposed Study of CHIV
Background:
The lesion is defined by a consensus to have clusters of monocytes in more than 5% of the intervillous space. The monocyte clusters should contain at least 80% monocytes. There may be heterogeneity in the distribution of intervillous monocytes. The lesion has an association with increased perivillous fibrinoid and villitis of unknown etiology. There is no clear association of obstetrical outcome with these histological features, although there is some evidence that monocytes filling more than 50% of the intervillous space are associated with more severe outcomes.
Associated clinical outcomes include a high incidence of fetal loss at all gestations, but greater in the first and second trimester, fetal growth restriction, and recurrence in multiple pregnancies. The growth restriction is often early onset and may be associated with oligohydramnios. There may be an elevation of maternal serum alkaline phosphatase above normal pregnancy values.
An immune origin of the lesion has been hypothesized. There may be an association with maternal autoimmune disease, especially anti-phospholipid syndrome, and with anti-HLA antibodies. The microvillous border of syncytiotrophoblast can be immunostained with c4d, a marker of antibody initiated fixation of complement.
Many treatment regimens have been used to prevent recurrent fetal loss, and anecdotally have resulted in a live born infant. These have included combinations of low dose aspirin, low molecular weight heparin, prednisone and hydroxychloroquine. No treatments have been demonstrated to be superior.
There is no standard pre-delivery method to diagnosis the lesion in an index pregnancy. Measures of early onset growth restriction are consistent with the lesion in pregnancies after a primary histologic diagnosis. The histologic lesions show variety and it is possible that the lesion is a common pathway of different etiologies. Only one, malaria, has been specifically identified. A better understanding of the pathogenesis of the lesion is needed.
The goal remains to find a specific test for the lesion prior to delivery, and an effective treatment. Even though the lesion is infrequent (less than .5% prevalence), it can cause recurrent fetal losses in some mothers.
Aims of the study
Part 1: Retrospective study of the histology:
1. Develop a quantifiable method of measuring intervillous monocytes, perivillous fibrin/fibrinoid, and VUE
2. Utilize CD 68, anti T cell, and c4d staining on cases and develop quantifiable measures.
3. Correlate with quantified measures with outcomes: first trimester fetal death, second trimester fetal death, third trimester fetal death, fetal growth restriction in the second trimester, fetal growth restriction in the third trimester, history of recurrent pregnancy loss, and history of recurrent CHIV. .
4. Correlate quantified histologic measures with treatment, and if possible, from placental samples from the same patient before and after treatment.
Part 2: Prospective study of mothers with a history of previous CHIV or with early onset severe fetal growth restriction.
1. Obtain maternal serum at first visit, at time of delivery, and before and after start of treatment to test for markers of the disease including alkaline phosphatase, serum complement panel, and red cell c4d.
2. Perform an auto-antibody panel including anti-phospholipid and anti-HLA.
3. Save serum to explore other markers of monocyte activation, syncytial trophoblast injury, or of auto/allo-antibodies to trophoblastic antigens
4. In addition to routine specimen processing, prepare tissue of further basic research on CHIV including frozen placental tissues, and monocyte extraction from placenta
Part 3: Prospective Clinical trial
Trial comparison of at least two therapy regimes against historical controls
Methods:
Part 1.1
The slides from cases of previously diagnosed CHIV are scanned and areas are selected that do not contain lesions or non-placental tissue. The size of the areas on each sample slide are calculated. The number of intervillous monocytes, foci of VUE, and area of pervillous fibrinoid are calculated for each area and summed area of each case. A shared software solution will be developed to use image analysis to perform this procedure. The range of values of the measured variables for each case in different slides of the same sample will also be recorded.
Part 1.2
From the same cases above, additional slides will be cut for immuno-staining with CD68, T-cell markers, and c4d along with controls. The same procedures will be usedused to select areas to evaluate as in part 1.1 . Then, software will be developed to count each of the CD68 cells in the intervillous space, the T-cells in the villi, and linear extent of c4d staining along the villous surface.
Part 1.3
The various histological outcomes will be compared to the major clinical outcomes, first trimester fetal death, second trimester fetal death, third trimester fetal death, fetal growth restriction in the second trimester, fetal growth restriction in the third trimester, history of recurrent pregnancy loss, and history of recurrent CHIV. Statistical analysis will look at independence of the variables, and the best cluster of variables to “predict” the clinical outcome and, if possible, using ROC analysis to create a diagnostic score.
Part 1.4
Using the best cluster of variables to “predict” outcome, the measure of these variables in the specimens before and after treatment in an individual patient are tested against the null hypothesis that treatment did not alter the diagnostic score.
Part 2.1
The serum values will be compared to controls without evidence of early growth restriction, or history of CHIV, and to cases with evidence of early growth restriction with and without the diagnosis of CHIV. The goal is to find a correlation of the serum markers with the diagnosis of CHIV
Part 2.2
These antibody screening will be from routine clinical laboratory procedures. The prevalence of such antibodies in CHIV will be calculated. In addition, cases with autoantibodies will be stratified in comparisons with obstetrical outcomes, measures of alloantigen response, and of treatment outcomes in part 3.
Part 2.3 and part 2.4
Future studies into the pathogenesis of the disease depend on researcher initiative. A sample proposed study that hypothesized an alloantibody to a paternal microvillous antigen, could utilize frozen section slides of placentas including those from the patients and controls. An Fc receptor blocker would be applied to the slides, and then CHIV and control serums applied to the slides. They would then be rinsed, and a fluorescent labeled anti-human IgG would be applied. Positive fluorescent staining would be evidence of specific anti trophophoblast antibody if the control serums were negative. Further studies could be designed to identify the antigen.
Part 3:
The high recurrence of fetal death in mothers with identified CHIV in a prior pregnancy precludes an untreated group given anecdotal reports of successful treatment. A panel of obstetricians would decide on the best way to approach comparing randomly assigned treatment groups. The results of the study would also be stratified by various anatomic and clinical pathological variables elucidated in parts 1 and 2.
References
1. Bos M, Nikkels PGJ, Cohen D, et al. Towards standardized criteria for diagnosing chronic intervillositis of unknown etiology: A systematic review. Placenta 2018;61:80-8.
2. Benirschke K, Kaufmann P. Pathology of the Human Placenta. Third ed. ed. New York: Springer-Verlag; 1995.
3. Russell P. Inflammatory lesions of the human placenta. III. The histopathology of villitis of unknown aetiology. Placenta 1980;1:227-44.
4. Labarrere C, Mullen E. Fibrinoid and trophoblastic necrosis with massive chronic intervillositis: an extreme variant of villitis of unknown etiology. Am J Reprod Immunol Microbiol 1987;15:85-91.
5. Valderrama E. Massive chronic intervillositis: Report of three cases. Lab Invest 1992;66:10P.
6. Jacques SM, Qureshi F. Chronic intervillositis of the placenta. Arch Pathol Lab Med 1993;117:1032-5.
7. Salafia CM, Ernst LM, Pezzullo JC, Wolf EJ, Rosenkrantz TS, Vintzileos AM. The very low birthweight infant: maternal complications leading to preterm birth, placental lesions, and intrauterine growth. Am J Perinatol 1995;12:106-10.
8. Salafia C, Maier D, Vogel C, Pezzullo J, Burns J, Silberman L. Placental and decidual histology in spontaneous abortion: detailed description and correlations with chromosome number. Obstet Gynecol 1993;82:295-303.
9. Redline RW, Zaragoza M, Hassold T. Prevalence of developmental and inflammatory lesions in nonmolar first-trimester spontaneous abortions. Hum Pathol 1999;30:93-100.
10. Boyd TK, Redline RW. Chronic histiocytic intervillositis: a placental lesion associated with recurrent reproductive loss. Hum Pathol 2000;31:1389-96.
11. Doss BJ, Greene MF, Hill J, Heffner LJ, Bieber FR, Genest DR. Massive chronic intervillositis associated with recurrent abortions. Hum Pathol 1995;26:1245-51.
12. Salafia CM, Cowchock FS. Placental pathology and antiphospholipid antibodies: a descriptive study. Am J Perinatol 1997;14:435-41.
13. Ordi J, Ismail MR, Ventura PJ, et al. Massive chronic intervillositis of the placenta associated with malaria infection. Am J Surg Pathol 1998;22:1006-11.
14. Leopardi O, Naughten W, Salvia L, et al. Malaric placentas. A quantitative study and clinico-pathological correlations. Pathol Res Pract 1996;192:892-8; discussion 9-900.
15. Hyde SR, Benirschke K. Gestational psittacosis: case report and literature review. Mod Pathol 1997;10:602-7.
16. Jacques SM, Qureshi F. Chronic chorioamnionitis: a clinicopathologic and immunohistochemical study. Hum Pathol 1998;29:1457-61.
17. Khong TY ME, Nikkels PGJ, Morgan TK, Gorgdijn SJ, ed. Pathology of the Placenta: A Practical Guide: Spinger; 2019.
18. Bendon RW, Coventry S, Thompson M, Rudzinski ER, Williams EM, Oron AP. Significance of C4d Immunostaining in Placental Chronic Intervillositis. Pediatr Dev Pathol 2015;18:362-8.
19. Freitag L, von Kaisenberg C, Kreipe H, Hussein K. Expression analysis of leukocytes attracting cytokines in chronic histiocytic intervillositis of the placenta. Int J Clin Exp Pathol 2013;6:1103-11.
20. Koby L, Keating S, Malinowski AK, D’Souza R. Chronic histiocytic intervillositis – Clinical, biochemical and radiological findings: An observational study. Placenta 2018;64:1-6.
21. Marchaudon V, Devisme L, Petit S, Ansart-Franquet H, Vaast P, Subtil D. Chronic histiocytic intervillositis of unknown etiology: clinical features in a consecutive series of 69 cases. Placenta 2011;32:140-5.
22. Nowak C, Joubert M, Jossic F, et al. Perinatal prognosis of pregnancies complicated by placental chronic villitis or intervillositis of unknown etiology and combined lesions: About a series of 178 cases. Placenta 2016;44:104-8.
23. Ongaro D, Terry J. Reproducibility of Grading in Chronic Intervillositis of Unknown Etiology. Pediatr Dev Pathol 2020;23:210-4.
24. Revaux A, Mekinian A, Nicaise P, et al. Antiphospholipid syndrome and other autoimmune diseases associated with chronic intervillositis. Arch Gynecol Obstet 2015;291:1229-36.
