Clinical determination of gestational age is more accurate the earlier in gestation that it is undertaken. In some cases prenatal obstetrical care is late or absent, and the autopsy determination of gestation is important in determining the relationship of growth to gestation. The factors that determine developmental progression are multiple and discrepancies in different aspects of gestational development can be a clue to underlying pathology. The autopsy can evaluate gestational development of internal organs including brain maturation as well as the usual clinical external and radiographic measures.
A. Introduction
The gestational age is an important baseline from which appropriate development is measured. Conventional gestational age is not from conception but from the first missed menstrual period, i.e. menstrual age. Term gestation is within 2 weeks of 40 weeks of menstrual age. The earlier in gestation, the more stereotyped is the growth and development, although chromosomal and genetic disease can delay growth. Perhaps the most important use of the gestational age is determining if the infant is appropriate, small or large for gestational age. Other organ development may also benefit by comparison to normal for the gestational age. Therefore establishing the gestation is an early critical step in the autopsy.
A reliable last normal menses date can be used to calculate the gestational age, but bleeding at implantation or irregular periods can cause errors. Some mothers may not be certain of the last menses. Others, for example parents with infertility using temperature charts for ovulation, may be very accurate. In many patients the gestational age determined by menses date is confirmed (or not) by an early gestational ultrasound. Later ultrasound estimates of gestation may be less accurate. If there was only a mid trimester ultrasound estimate of gestation, our maternal serum screening laboratory accepted the menstrual dates if they were within two weeks of the mid trimester ultrasound, otherwise we used the ultrasound estimate. The obstetrical chart will usually record the best obstetrical estimate of the gestational age. In cases with limited or absent obstetrical care, the recorded gestational age may be based on a late ultrasound study or on the weight of the infant at birth. These estimates can be very wrong.
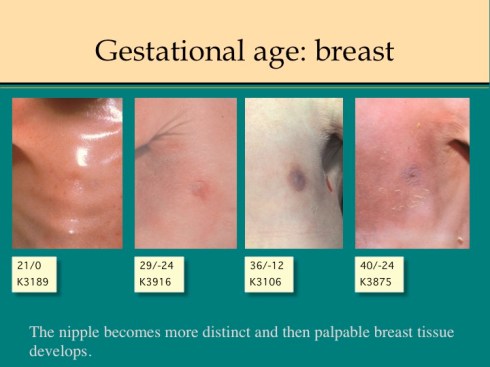
External physical features mature with gestation [1]. These changes are routinely used to estimate gestation in the nursery following the template proposed by Dubowitz. We use the revised Ballard score which has been validated from 20 to 44 weeks of gestation [2][3]. The score is divided into a neuromuscular maturity portion and a physical maturity portion. The latter portion can be performed postmortem, although portions may be compromised by prolonged postmortem retention. The resulting score must be doubled to use the table of correlation with gestational age. In the nursery, the scoring is accurate to within 1 week, but this may not be true of the postmortem physical score, and a reasonable estimate is that the score is correct within +/- 2 weeks.
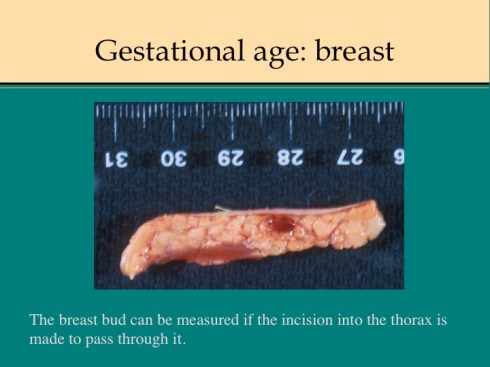
The estimate of breast bud size in the score can be replaced by the measurement of the breast tissue during dissection.
The internal development of organs is another method to determine gestational age. The brain gyration pattern has the most discrete changes over a wide gestational age range. Microscopically, the kidney, lung, skin, testes and brain have developmental landmarks in that can be used, if not to determine, at least to confirm the expected degree of development for gestation. Radiological development of ossification zones also mark gestational age.
The gestational age in fetuses less than 20 weeks can be estimated from fetal size using the crown rump length and/or the toe to heel length. There are complex techniques as well for embryonic staging, but the size is usually adequate. At these early gestations, the time retained in utero since fetal death must also be accounted for when comparing with the clinical estimate of gestational age at birth.
Even at early gestation disease may influence fetal size for gestation. The goal of the autopsy is to integrate all of the available clinical and anatomic evidence to determine gestation, and to account for variation due to pathology.
B. The external Ballard score:
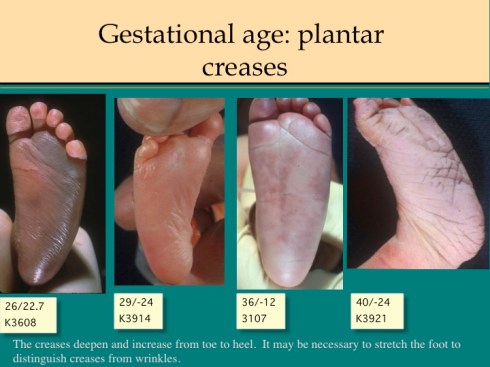
The earlier published observations of Farr are helpful in fleshing out the detail of the Ballard score. For skin, the Ballard score evaluates skin texture and opacity. Farr comments that cracking is especially evident on the hands and feet, and that opacity can best be evaluated on the trunk. Farr recommends examining the back for lanugo, holding the infant up to the light. Lanugo is the fine, weakly pigmented baby hair, not later mature hair. The trick to observing the plantar flexion creases, as noted by Farr, is to stretch the sole from heel to toes and note the creases that persist. Farr estimated breast tissue by palpating between finger and thumb. Farr evaluated the curvature of the upper part of the pinna above the external meatus as: “0” is almost flat, “1” is incurving of any degree of any portion, “2” is partial incurving of the entire upper pinna, and “3” is well defined incurving of the entire pinna. The Ballard score evaluates recoil of the pinna, but this can be superimposed on the Farr scoring system. Ballard adds scoring of eyelid fusion for earlier gestation. The genital changes are self-explanatory.






Some pathologic conditions may modify the score, for example oligohydramnios may result in compression of the pinna and severe growth restriction may reduce subcutaneous fat sufficiently to delay the expansion of the labia majora. Maceration may result in complete loss of the epidermis, making veins invisible from diffused hemoglobin, or opening previously sealed eyelids. If a score for a particular feature is not consistent with the evaluation or cannot be evaluated, the mean score of the other features can be substituted to estimate the gestational age.
C. Measurement of crown rump and foot length
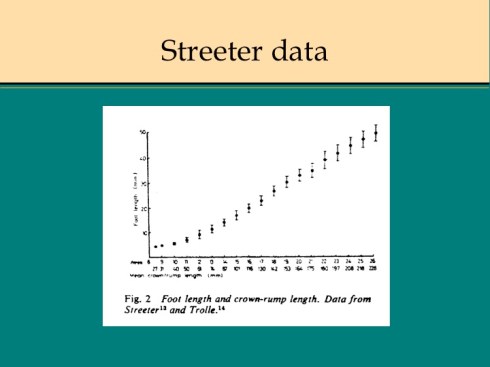
For fetuses less than 20 weeks gestation, the simplest estimate of gestational age is to use the measurement of the foot length (heel to toe) and crown rump. Usually at least one of these measurements is possible. The measurement of crown rump is more complicated in these specimens as vaginal ultrasonography has demonstrated [4]. In the older fetus, the measure is truly crown to rump, but in the more embryonic specimen the longest longitudinal measure is the best approximation. The relationship of foot length has been confirmed in multiple anatomic and ultrasound studies [5][6, 7]. If the fetal foot is placed firmly on the ruler, the measurement can be read directly. A useful composite chart, using data of Streeter and Trolle to determine gestation from these measurements, was published by Berry [8]. In the embryonic specimen, gestational age can also be determined by the appearance of development features, particularly of the heart, brain and body [9][10, 11]. Ultrasonography can detect similar anatomic landmarks, in addition to functional ones [12].
D. Gyral development of the brain:
The gross development of the gyri of the cerebral cortex provides another marker of gestation. Larroche pioneered this approach, and in 1977 two further studies validated it. One study was meticulously detailed, and studied 507 brains. The dating was based on last menstrual period, and any error in dating was eliminated statistically by using approximately 2 week intervals during which either 25 or 50% of cases demonstrated the feature to 75-100% demonstrated the feature [13]. The published study included diagrams and detailed descriptions. The second study looked at 80 brains, and used menstrual dates and renal histology to assign gestation [14]. The latter cryptically was stated as “Conversely, in the kidneys it was comparatively easy to count layers of completed glomeruli. At 23 weeks, three layers were seen. These increased weekly by one, so that by 30 weeks ten layers had formed. Thereafter, glomerulogenesis became patchy.” The validation for this renal technique was not presented. The authors published a very clear series of lateral and medial photographs of the brain in 2 week intervals from 22-40 weeks of gestation. As they suggested, posting this chart in the morgue makes it very easy to assign a brain visually to one of the intervals.

E. Bone changes with development
The progressive development of radiologically detectable ossification centers has been correlated with gestational age. This may be particularly helpful in determining gestation in the dismembered fetus or in fetus papyraceus. For example, clinical ultrasound detects ossification centers in the calcaneus and talus in all fetuses by 22 weeks [15]. Berry provided a chart of the appearance of vertebral body centers in which cervical and sacral vetebra can help determine gestation in fetuses less than 15 weeks [8]. Using the hand and foot bones, the range may be extended up to 20 weeks, although this would require high resolution radiographs of the extremities [16]. The middle phalanges of the toes in general ossify after 19 weeks gestation. In very macerated or decomposed infants, careful measurements of the bone may identify gestation and pathology, e.g. abnormal cranial bone size for gestation. Detailed post mortem bone measurements are recorded in a monograph by Fazekas and Kósa, but this work is not readily available [17].
F. Microscopic changes with gestation
1. Kidney:
The cessation of glomerulogenesis in the nephrogenic (subcapsular zone) of the kidney is a useful marker of maturation. Originally believed to correlate best with fetal size, a subsequent study confirmed that nephrogenesis ceases at 35 weeks gestation [18, 19]. As mentioned in a study of brain maturation, counting generations of glomeruli may also be used to estimate gestational age, but I have no experience with this.
2. Lung
Descriptively, there is also a regular progression of microscopic features. The glandular stage form 10 to 16 weeks of gestation is followed by a cannalicular period up to 24 weeks gestation during which time capillaries begin to approach the airway epithelium, and finally a progressive development of the terminal sacs with progressive thinning of the epithelium and protrusion of capillaries. Multiple morphometric measures of the lung, such as volume proportion of air spaces, have good correlation with gestational age [20]. A simple quantitative method to estimate gestation from the lung is the radial alveolar count which is exponentially related to gestation after 18 weeks [21].
3. Brain
The brain has many progressive features such as the thickness of the molecular layer in the vermis that could be used to estimate gestation [22].
4. Skin
A sample of skin that includes the breast bud and the full thickness of subcutaneous fat can be used to confirm the features of skin, breast, and lanugo utilized in the Ballard score. The thickening of the epidermis, the progression of hair development and the size of the breast bud can be evaluated. This has not been reported as an independent method of determining gestation.
5. Testes
By 29 weeks all testes should have 2 layer tunica albuginea[23]
G. Interpretation
An infant may have a low birth weight for gestational age that may due to utero-placental ischemia or intrinsic disease of the fetus or placenta. A potential pitfall for the pathologist is that the concept of intrauterine growth retardation includes infants who have fallen below the expected intrauterine growth curve as determined by ultrasound even if such infants still have normal for gestation birth weights. Large for gestation infants have a different differential diagnosis including maternal diabetes, hydrops (anasarca) or rare gene conditions. The value of postmortem estimation of gestational age is exemplified in the case of a 1,290 g, stillborn infant delivered at home. The gestation was unknown, but based on birth weight had been clinically assigned as 30 weeks. The placenta demonstrated chorioamnionitis. The postmortem Ballard score examination concluded that the infant was near term (K2978, K2979). This implied that the infant was severely growth retarded, and must therefore have had disease in addition to the chorioamnionitis.
Once the gestational age is established, other features such as brain, kidney and lung development should be at the same gestational development. If all of these features are greater or lesser than the estimated gestation, the basis of the gestational age should be reevaluated. If a single feature is not consistent, there may be organ disease, for example delayed gyral development with brain disease or low alveolar radial count with pulmonary hypoplasia.
H. Reference
- Farr V, Mitchell RG, Neligan GA, Parkin JM: The definition of some external characteristics used in the assessment of gestational age in the newborn infant.Develop Med Child Neurol 1966,8:507-511.
- Dubowitz L, Dubowitz V, Goldberg C: Clinical assessment of gestational age in the newborn infant.J Pediatr 1970,77:1-10.
- Ballard J, Khoury J, Wedig K, Wang L, Eilerswalsman B, Lipp R: New Ballard Score, expanded to include extremely premature infants.J Pediatr 1991, 119:417-423.
- Goldstein S: Embryonic Ultrasonographic Measurements – Crown-Rump Length Revisited.American Journal of Obstetrics and Gynecology 1991, 165:497-501.
- Streeter GL: Weight, sitting height, head size, foot length, and menstrual age of the human embryo.Contrib Embryol Carnegie Inst 1920, 11:143-170.
- Mercer BM, Sklar S, Shariatmadar A, Gillieson MS, D’Alton ME: Fetal foot length as a predictor of gestational age.Am J Obstet Gynecol 1987, 156:350-355.
- Dolhay B, Batar I, Papp Z: Correlation of the distance between the heel and big toe with the weeks of gestation, biparietal diameter, and body weight.Am J Obstet Gynecol 1973,117:1142-1144.
- Berry CL: The examination of embryonic and fetal material in diagnostic histopathology laboratories.J Clin Path 1980, 33:317-326.
- Moore GW, Hutchins GM, O’Rahilly R: The estimated age of staged human embryos and early fetuses.Am J Obstet Gynecol 1981, 139:500-506.
- Sissman NJ: Developmental landmarks in cardiac morphogenesis: comparative chronology.Am J Cardiol 1970, 25:141-148.
- O’Rahilly R, Müller F, Hutchins GM, Moore GW: Computer ranking of the sequence of appearance of 100 features of the brain and related structures in staged human embryos during the first 5 weeks of development.Am J Anat 1984, 171:243-257.
- Warren WB, Timor-Tritsch I, Peisner DB, Raju S, Rosen MG: Dating the early pregnancy by sequential appearance of embryonic structures.Am J Obstet Gynecol 1989, 161:747-753.
- Chi JG, Dooling EC, Gilles FH: Gyral development of the human brain.Ann Neurol 1977, 1:86-93.
- Dorovini-Zis K, Dolman CL: Gestational development of brain.Arch Pathol Lab Med 1977, 101:192-195.
- Goldstein I, Reece EA, Hobbins JC: Sonographic appearance of the fetal heel ossification centers and foot length measurements provide independent markers for gestational age estimation.Am J Obstet Gynecol 1988, 159:923-926.
- Kjar I: Skeletal maturation of the human fetus assessed radiographically on the basis of ossification sequences in the hand and foot.Am J Phys Anthrop 197, 40:257-276.
- Fazekas IG, Kósa F: Forensic Fetal Osteology.Budapest: Akadémiai Kiadó; 1978.
- Potter E, ST T: Glomerular development in the kidney as an index of fetal maturity.J Pediatr 1943, 22:695-706.
- Fujikura T, Froehlich L: Birthweight, gestational age, and renal glomerular development as indices of fetal maturity.Am J Obstet Gynecol 1972, 113:627-631.
- Langston C, Thurlbeck WM: Lung growth and development in late gestation and early post natal life.Persp Pediatr Pathol 1982, 7:203-235.
- Cooney T, Thurlbeck W: The radial alveolar count method of Emery and Mithral: a reappraisal 2- Intrauterine and early postnatal growth.Thorax 1982, 37:580-583.
- Friede RL: Dating the development of human cerebellum.Acta Neuropathol (Berl) 1973, 23:48-58.
- Waters B, Trainer T: Development of the human fetal testis.Pediatr Pathol 1996, 16:9-23.
