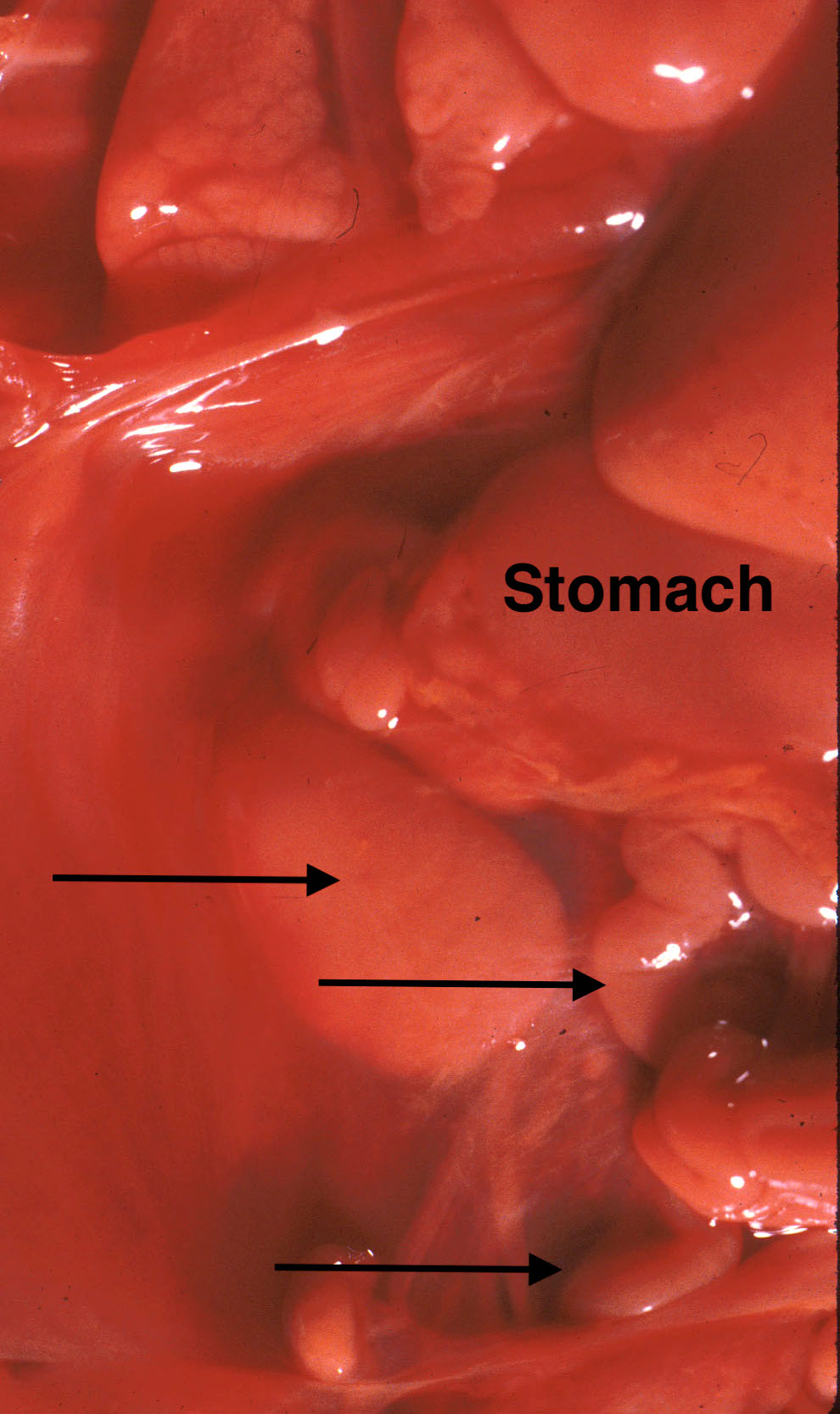
The spleen is easily located along the left edge of the stomach. Looking at the organ from the posterior, the tail of the pancreas reaches to it. By lifting the tail, pancreas can easily be dissected free toward the duodenum. The spleen is occasionally malformed, for example trisomy 13, or demonstrates small splenules at the splenic periphery. In heterotaxy syndromes, there may be asplenia or polysplenia, and the multiple spleens are often on the right side of the body1 (Fig 1).
Fig 1a: The stomach is on the right side of the abdomen, and the arrows point to multiple spleens in this infant with polysplenia syndrome with bilateral left lungs and cardiac malformation. The infant was 20 weeks of gestation with prolonged retention. Fig1 b: Multiple spleens can be seen microscopically in this 19 weeks of gestation infant with polysplenia syndrome with situs inversus and complex cardiac malformations. The infant had 12-24 hours of postmortem retention.
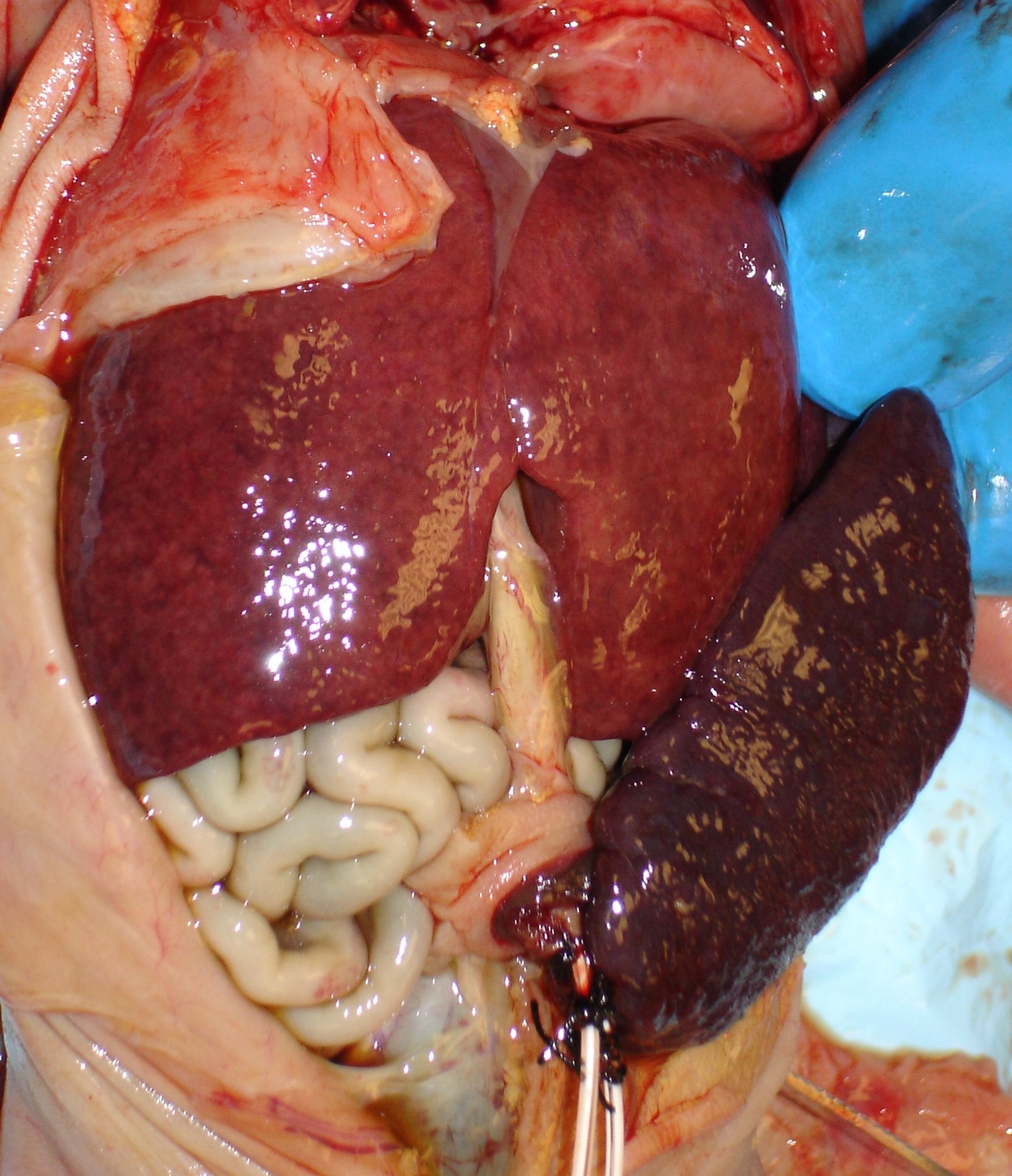
The most common gross abnormality is enlargement. There may be increased size/weight from passive congestion with heart failure, but it is lymphoid hyperplasia from blood borne fetal infection that produces gross splenomegaly (Fig 2). The average spleen to brain weight ratio is 0.022. The spleen can easily be removed and weighed. A flat longitudinal sample maximizes the histologic area.
Fig 2: The abdomen shows hepato-splenomegaly in a 26 weeks of gestation infant with congenital CMV infection, who survived 24 hours.
Microscopic Examination:
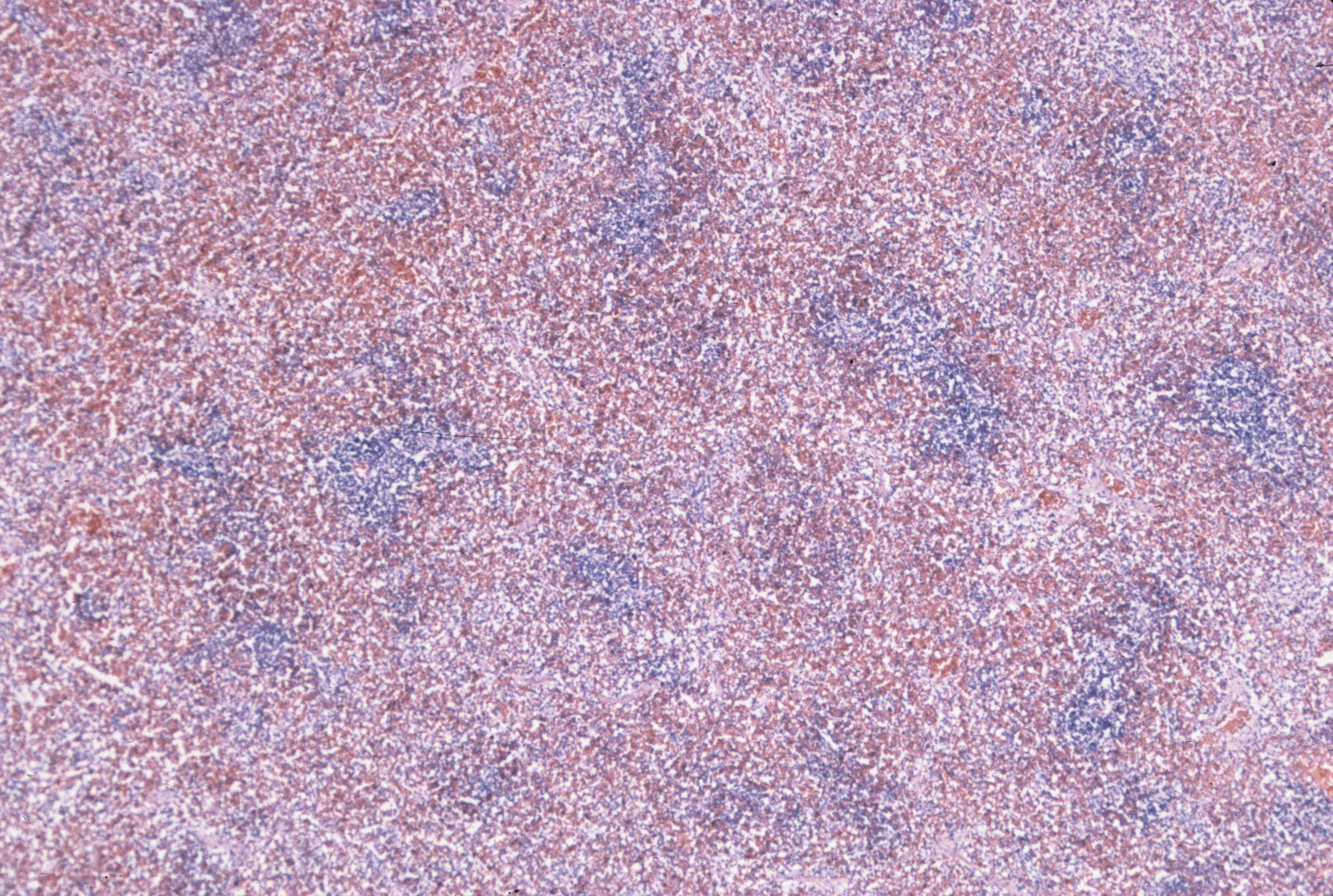
Lymphoid tissue: The normal fetal spleen demonstrates a cuff of predominantly T lymphocytes around the arterioles (Fig 3a, b).
Fig 3a: A cuff of basophilic lymphocytes can be seen around an arteriole in this spleen from a 39 weeks of gestation infant with failed resuscitation due to fetal akinesia sequence. (20x, H&E)Fig 3b: The lymphocyte cuffs can be seen around the spiral arteries in this 32 weeks of gestation infant with acute asphyxia and 6 hours of intrauterine postmortem retention. (4x, H&E)
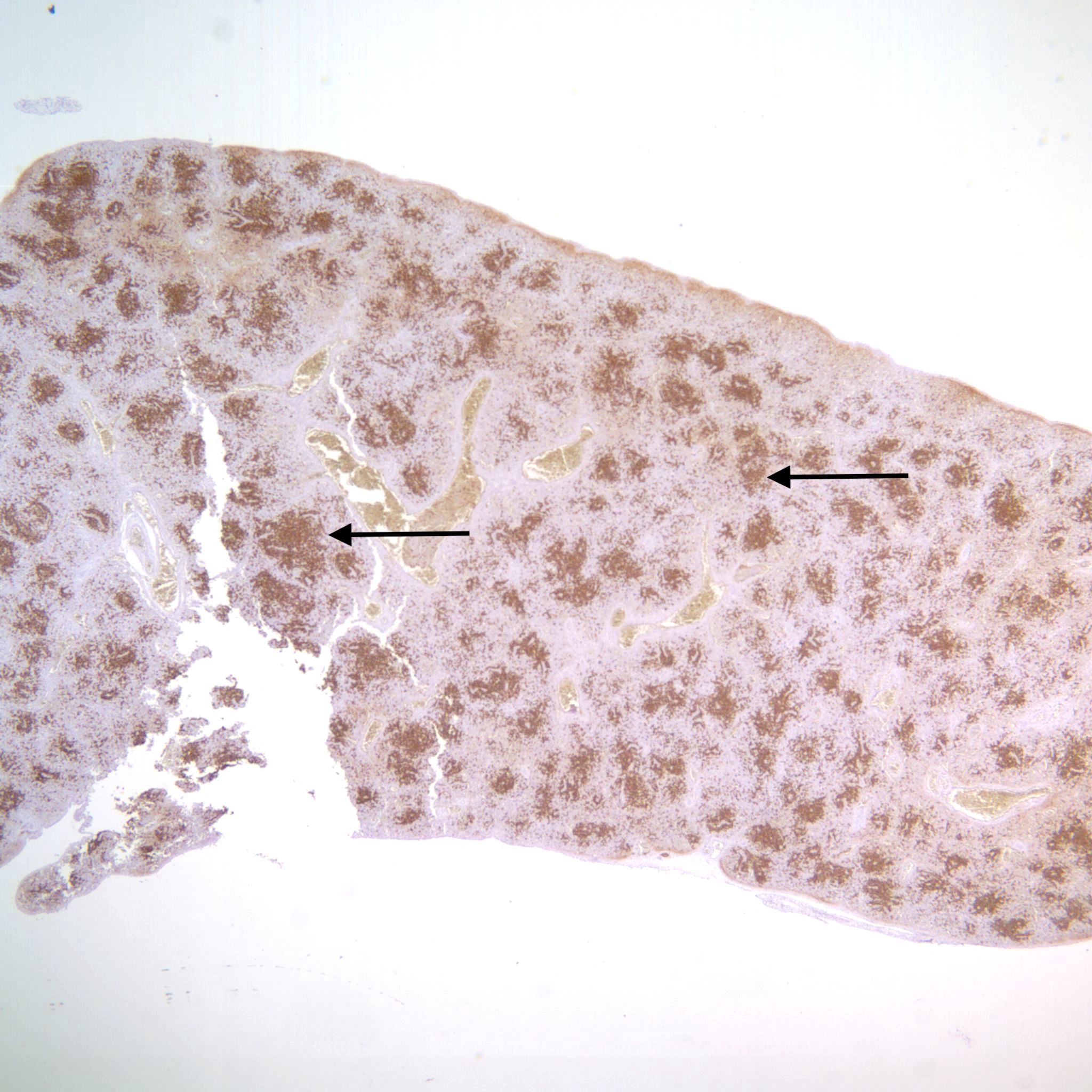
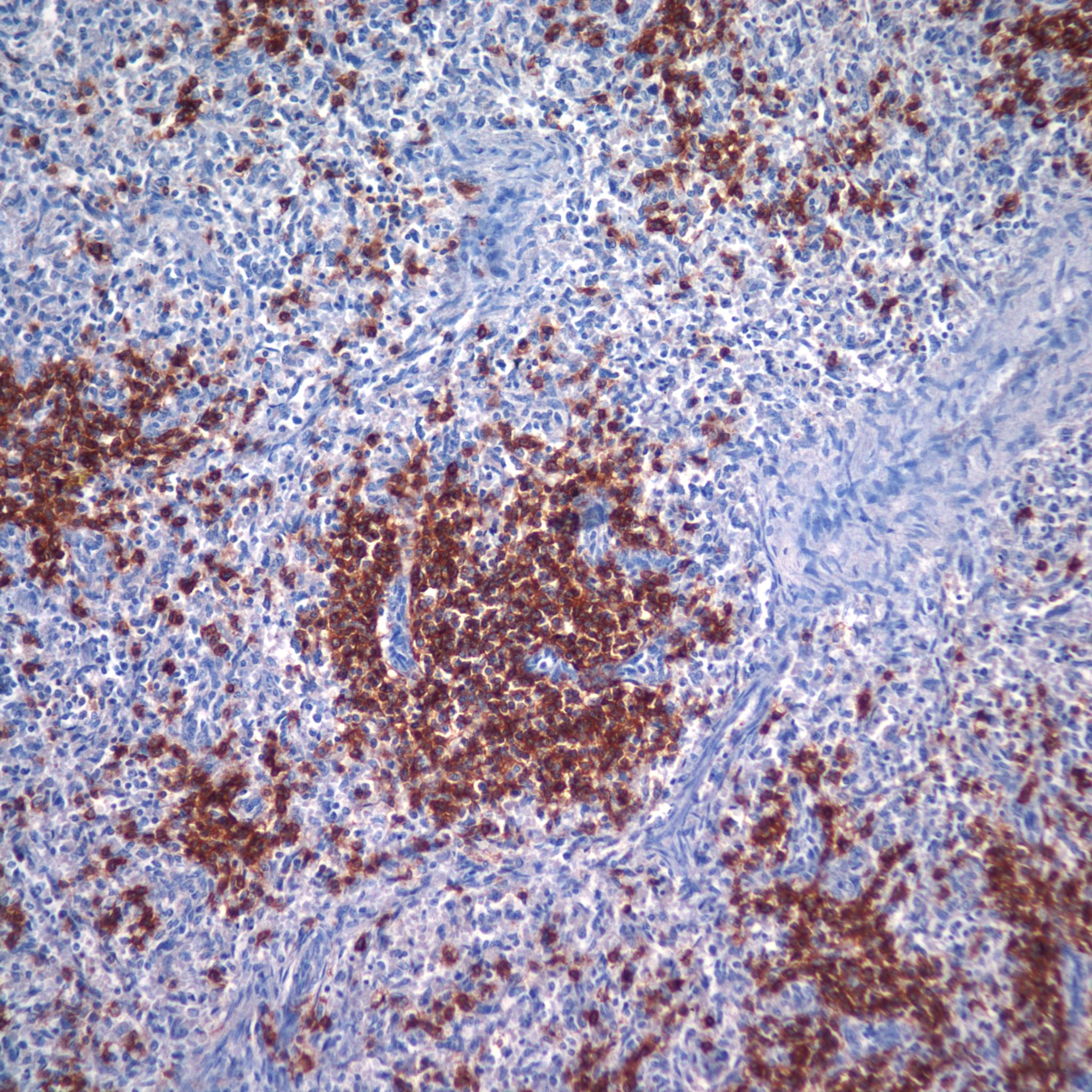
With antigenic stimulation, B lymphocytes proliferate usually eccentric to the T cell cuffs. (Fig 4a, b)
Fig 4a: This slide is stained for B-cells (brown stain) which are increased. The arrows point to the expansion of the B-cells eccentrically to the arterial cuff. This 22 weeks of gestation infant with premature rupture of membranes and chorioamnionitis had beside B-cell proliferation in the spleen, complete thymic involution, pneumonitis, and white matter necrosis. A postmortem lnung culture did not grow bacteria. The infant survived 45 minutes. (2x, CD20)Fig 4b: The proliferation of B cells (brown stain) beyond the usual arterial cuff of lymphocytes is present. This 22 weeks of gestation infant was an intrapartum death following preterm labor. There was a grade III intraventricular hemorrhage in the brain, but no evidence of intrauterine or fetal infection. There was also an acute subcapsular liver hematoma and skin bruising. There were no studies of platelet antigens. (20x, CD20)
With HSV infection in the spleen, there may be intense proliferation of B-cells (Fig 5).
Fig 5: There is a proliferation of more pleomorphic lymphoid cells rather than the normal small lymphocytes around arterioles. In other areas, the spleen demonstrated geographic necrosis with herpes simplex inclusions. This 29 weeks of gestation infant died of complications of congenital HSV infection at 24 hours of life. (40x, H&E)
It is unclear whether stress induced fetal cortisol reduces the T cell population in the spleen, as it does in the thymus. An interesting possibility is that some foreign antigens, for example from maternal cells, could be presented in the thymus and result in clonal suppression of T cells with receptors for these antigens. Possibly the innate immune system overrides this risk for microbial antigens.
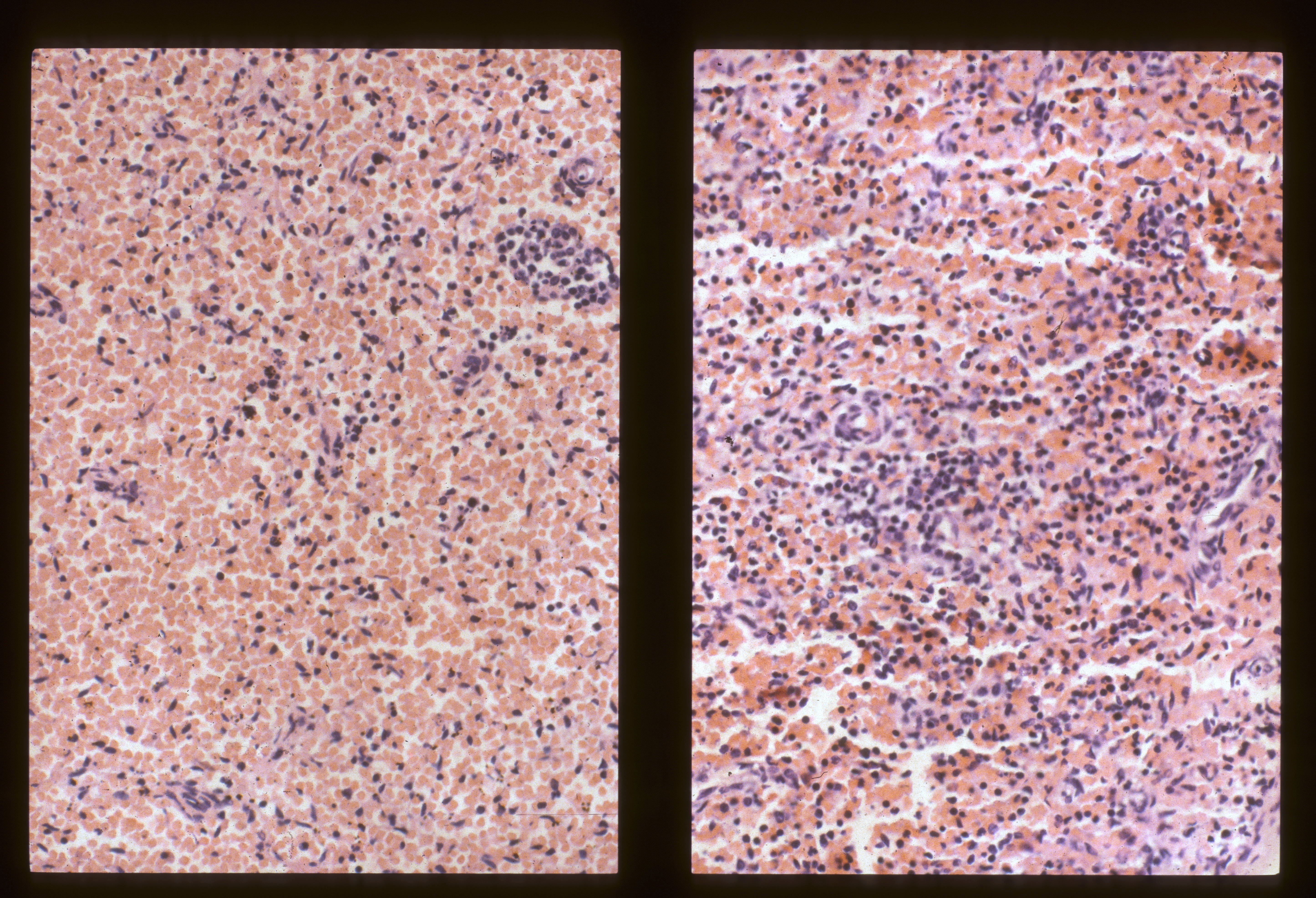
Red pulp: The sinuses may be congested, and conversely in fetal anemia, they may be notably empty. (Fig 6a, b).
Fig 6a: This image compares the spleen in acute twin-to-twin transfusion. The twin in the left panel is the recipient of the acute transfusion and shows the sinuses distended with blood compared to the sibling. The twins were 33 weeks of gestation with 12-24 hours of postmortem retention. (20x, H&E)Fig 6b: This spleen demonstrates an almost complete absences of red cells in the sinuses except for some probably nucleated red cells, mixed with leukocytes. The infant died from fetal to maternal hemorrhage at 27 weeks of gestation followed by 48-96 hours of postmortem retention. There were multiple intervillous thrombi in the placenta and a family history of Marfan’s disease. (40x, H&E)
With immune hemolysis, the reticulo-endothelial system of the sinuses is responsible for phagocytosis of the antibody targeted red cells. This results in hemosiderin in the RE cells lining the sinuses. This observation was made first by Larroche in cases with Rh allo-immunization2 (Fig 7a, b).
Fig 7a: This image shows scattered hemosiderin iron positive (blue) macrophages in the splenic sinuses. The explanation of the presumed phagocytosis of red cells was unclear as this 41 weeks of gestation infant was not anemic, but had systemically distributed petechiae including the skin. Death was attributed to a complete placental separation 4 to 12 hours prior to delivery. (40x, iron)Fig 7b: This image shows many iron containing cells (blue) in the splenic sinusoids. This 34 weeks of gestation infant had a mildly enlarged spleen and died at 6 hours of age. Death was from fetal akinesia sequence associated with congenital CMV (inclusions in multiple organs) and periventricular glial scarring. The hemophagocytosis was speculated to be due to endothelial injury to red cells from the CMV infection. (20x, iron)
The RE system may also show phagocytosis of targeted white blood cells, hemophagocytic lymphohistiocytosis (HLH) (Fig 8).
Fig 8: The splenic sinuses show phagocytosis of red and white blood cells (arrows). The infant was an intrapartum death at 22 weeks of gestation having hydrops of undetermined etiology. There was massive hepatomegaly with similar hemophagocytic lymphohistiocytosis (HLH) and increased erythropoiesis. The skin had numerous small capillary proliferations in the dermis. Primary HLH could not be excluded as genetic studies were not available. (40x, H&E)
Mass lesions: Splenic hamartomas may or may not be evident grossly, but microscopically they are well demarcated from the normal architecture of the spleen (Fig 9).
Fig 9a: This image demonstrates to demarcated splenic hamartomas (arrows). This 28 weeks of gestation infant died at 2 hours of age from the pulmonary hypoplasia from fetal hydrops of unknown etiology. Hamartomas are usually incidental findings. (2x, H&E)Fig 9b: This is higher magnification of the hamartoma in Fig 9a. (10x, H&E)
Other: Bacteria that reach the blood stream may result in postmortem gas production, and the spleen perhaps because it captures bacteria, may show gas bubbles (Fig 10).
Fig 10: The arrows point to gas bubbles in the spleen. This 27 weeks of gestation infant had more than 96 hours of postmortem retention. The placenta had multiple infarctions. (10x, H&E)
The fetal spleen can infarct with fetal anoxia3 (Fig 11).
Fig 11: This image shows a clear comparison of the infarcted spleen on the right compared to the normal spleen on the left. This 35 weeks of gestation infant had 12-24 hours of postmortem retention. The underlying cause of death was exsanguination from an umbilical cord ulcer. (2x, H&E)
References:
1. BH L. Five syndromes (malformation complexes) of pulmonary symmetry; congenital heart disease; and multiple spleens. Pediatr Pathol 1984;2:125-151.
2. Larroche JC. Developmental Pathology of the Neonate: Excerpta Medica; 1977.
3. Gosseye S, Golaire M-C, Larroche J-C. Cerebral; renal; and splenic lesions due to fetal anoxia and their relationship to malformations. Develop Med Child Neurol 1982;24:510-18.