A. Introduction
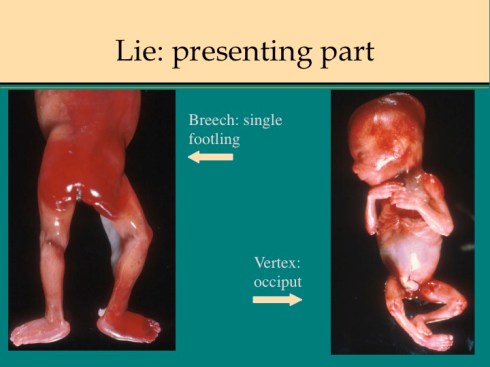
The fetal lie refers to the body axis position in utero (vertex, breech or transverse). The presenting part is the fetal tissue that first enters the cervical os. If the part remains within the constricting cervix, the pressure may occlude venous return resulting in distal erythema and edema. In mid-gestation deliveries, the cervix may not completely dilate and fetal parts are more frequently entrapped. If the presenting part can be identified, the lie can often be deduced. In a vertex lie, the brow or more commonly the occiput will present. A frank breech demonstrates a buttock presentation, and a footling breech presents one or two legs. An arm presentation may be vertex (i.e. alongside the head), or a transverse lie.
B. Determining fetal lie and presenting part
The presenting part in most cases can be identified by marked edema and erythema confined distally to a plausible line of constriction. Previable fetuses may have numerous ecchymoses that obscure evidence of the presenting part. An older infant may have only palpable scalp edema as evidence of a vertex presentation. The anatomic evidence of presentation should correlate with the obstetrical record. (Fig 1,2)

C. Long bone fracture
Fractures may occur during delivery. Those of long bones may show angulation or hematoma. The fracture can be confirmed on a full body radiograph. (Fig 3)
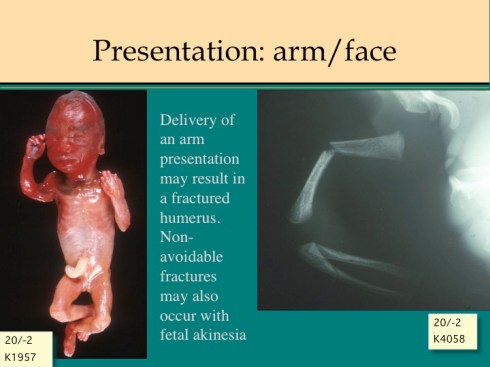
In previable infants, fractures may be the result of delivery of a fetus with a transverse lie or arm presentation and are not significant. Fractures in older infants need to be correlated with the delivery record of obstetrical manipulations, difficult delivery (which may be vaginal or Cesarean), and even potential causes of neonatal trauma. Fracturing the clavicle may be intentional with the delivery of an infant with shoulder dystocia. Osteogenesis imperfecta may account for fractures when there is no history of trauma (or even if there is).
D. Cervical spine fracture
Cervical fractures usually occur during vaginal delivery of breech presentation. In premature breech infants, the small body delivers through an incompletely dilated uterine cervix, which then clamps down on the neck. In an older infant, the after-coming head may be trapped by the pelvic outlet. Delivery of an entrapped head may fracture the neck from forceful traction and hyperextension. Either the fracture or asphyxia from the entrapment may cause death. Cervical fractures or dislocations may demonstrate elongation of the neck. Careful evaluation of the neck radiographs, spinal cord, and gross vertebra may be needed to detect the fracture or dislocation. On a radiograph, the cervical fracture may show only a small displacement from the smooth line of vertebral bodies. (Fig 4)
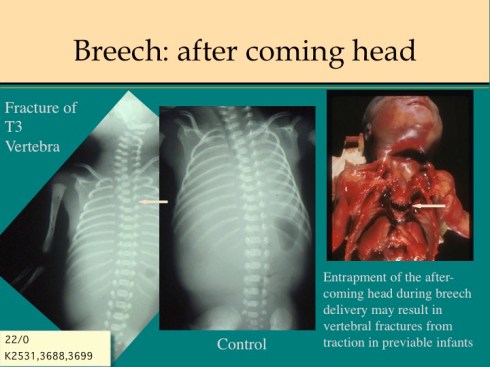
The “cervical” fracture may even occur in the upper thorax. The autopsy should carefully document a fracture, and interpret the significance in the context of the clinical history.
Previable fetuses are often breech, often delivered through an incompletely dilated cervix, and are inherently fragile. The obstetrician must deliver the previable fetus with the least morbidity to the mother, and may accept any fetal trauma as necessary. In extreme cases decapitation may be necessary to deliver a previable fetus.
E. Scalp hemorrhages
The infant’s head may have a palpable asymmetric enlargement due to hemorrhage. The most common is caput succedaneum, scalp edema from pelvic pressure on the presenting head. This is usually boggy to palpation. A scalp incision will expose subcutaneous hemorrhagic edema, but not a hematoma or free hemorrhage. Caput is often associated with cranial molding that elongates the head to permit delivery. Both result from the force of labor on a head that is relatively large for the maternal pelvic outlet. The cranial molding and caput are usually not a source of morbidity or mortality, although in the extreme there may be cranial injury.
Larger subcutaneous hemorrhage may occur. Coagulation abnormalities could underlie some larger hemorrhages. One cause of subcutaneous hemorrhage is prolonged application of a vacuum suction extractor. If applied for an extended time, vacuum extractors have caused hemodynamically significant blood loss [1].
More commonly significant are hematomas that occur beneath the aponeurosis of the scalp. There are no blood vessels in this area; therefore, the most likely source of blood is from a fracture of the skull with subperiosteal blood rupturing through the periosteum [2]. Over hours, such hemorrhages may cause hemodynamically significant fetal blood loss.
Blood draining from the ear canal may be evidence of basilar skull fracture. This can occur from improper application of obstetrical forceps. Part of the evaluation of lie and presentation is noting any bruising or lacerations that identify the location of forceps application, electrode placement or blood sampling applied to the presenting part.
The findings discussed above will generally be detectable as part of a systematic external examination, but there is value in integrating them with the lie, presentation, and clinical complications of delivery.
F. References:
- Benaron, D.A., Subgaleal hematoma causing hypovolemic shock during delivery after failed vacuum extraction: a case report.J Perinatol, 1993. 13(3): p. 228-31.
- Zelson, C., S.J. Lee, and M. Pearl, The incidence of skull fractures underlying cephalhematomas in newborn infants.J Pediatr, 1974. 85(3): p. 371-3.
