Clinical History: This infant was delivered to a 23 year old G2, P0 mother at 40 weeks gestation. The mother had good prenatal care with normal screening studies and no complications. She was admitted in labor at approximately 4:15 PM. Review of the fetal heart rate monitor did demonstrate a 10-12 minute episode of bradycardia which recovered with retention of good variability. It was attributed to an episode of uterine hyperstimulation. She was transferred from triage to a labor room at approximately 9:30. The fetal heart rate was 80-90 (maternal pulse 106) and decreasing. She was transferred to the OR at 9:45. The fetal heart rate was in the 60-70 range. After general anesthesia, the infant was delivered by Cesarean section by 9:55. The infant had 0 Apgar scores. Neonatology was present but could not resuscitate the infant. The umbilical cord arterial gas was pH 6.86, with a base excess of -19.8, pO2 of 8, and pCO2 of 113. The venous cord gas was pH 7.20, pO2 44, pCO2 54, and BE-8.5.
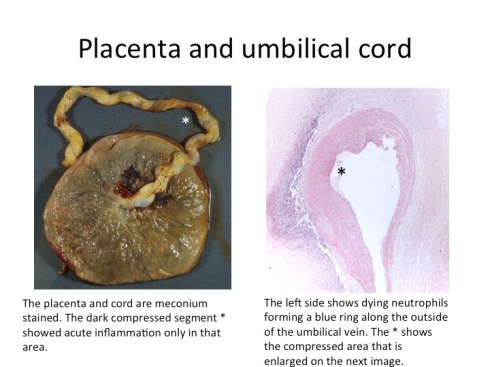
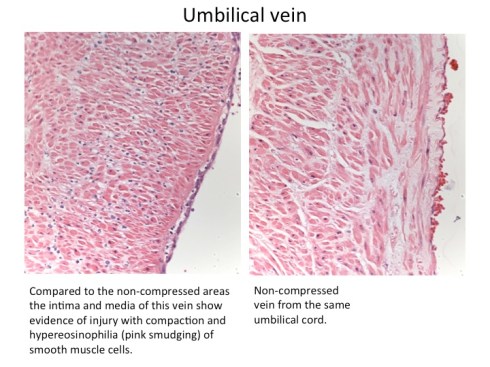
Placental Findings: The placenta was meconium stained including the umbilical cord. There was a narrowed area of darker thinner umbilical cord approximately 4 cm long near the middle of the cord. The cord was 54 cm long. The placenta weighed 470 grams. The compressed area of the cord demonstrated a crescent of neutrophils, many necrotic between the surface and the umbilical vein. The vein also demonstrated scattered neutrophils in the wall. Away from the compressed area there was no inflammation in the umbilical cord. The fetal membranes demonstrated pigment macrophages from the amnion to the decidua. There were no other signs of umbilical cord compression such as fetal vascular thrombi or stem vessel dilatation.
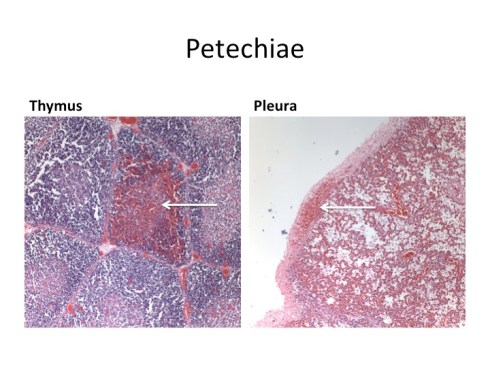
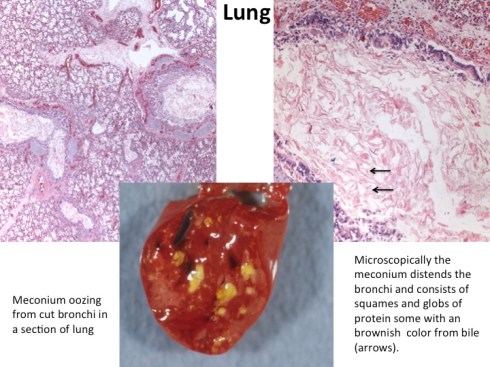
Autopsy findings: The autopsy was limited to the thorax. This was an appropriate weight term infant without evidence of intrauterine postmortem retention. The lungs extruded meconium from cut bronchi. There were sparse thymic and pleural petechiae. There were no subcutaneous edema or body cavity effusions. The thoracic organs were of appropriate weight without abnormality. The microscopic examination demonstrated bronchi distended with meconium, and confirmed the petechial hemorrhages.
Discussion: The cord blood gases show placental perfusion was continuing but that the fetus was still acidotic because fetal circulation was still occluded at the time of delivery. The source of the occlusion was anatomically evident in the umbilical cord. This is uncommon as most acute umbilical cord occlusions do not produce persistent gross compression. The history of at least one documented episode of bradycardia suggests repetitive umbilical cord compression. The development of umbilical vein inflammation and the depth of meconium macrophages suggests at least hours of repetitive compression. The autopsy findings demonstrated an acute asphyxia event as the immediate cause of death with evidence of gasping (meconium aspiration and intrathoraic petechiae) without evidence of chronic stress or injury, in that is there was no evidence of thymic involution or of pleural and pericardial effusions or other evidence of heart failure. The implication is that the earlier cord compressions did not cause fetal injury. This is consistent the clinical report that the initial observed episode of bradycardia resolved with good heart rate variability. However, it cannot be assumed that there were no consequences to the fetal brain. Unfortunately we were no permitted to examine the brain.
This case does leave many questions open, including the significance of the severe inflammatory umbilical in respect to prior compressions of the cord before the lethal event. The role of the rushing to Cesarean section and maternal anesthesia versus discovering and perhaps relieving the cord compression in improving the chance of fetal survival seems worth more discussion