Gross:
Color: The fetal liver is red without the brown lipofuscin that characterizes older livers. Some of the red may also be due to the prominent erythropoiesis in gestationally less mature livers. The color may be a deep red with liver sinusoidal congestion. The liver will become pale with fetal anemia, but yellow appearing livers can also be the result of storage diseases, some of which produce fetal ascites.
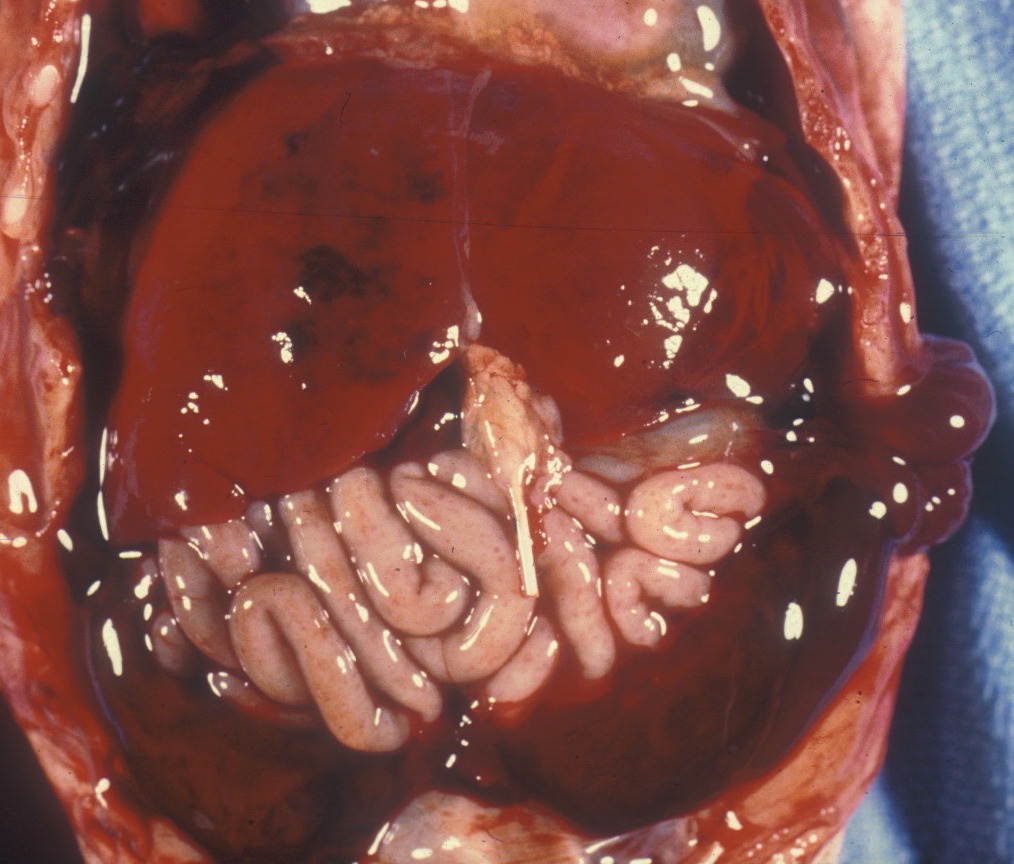
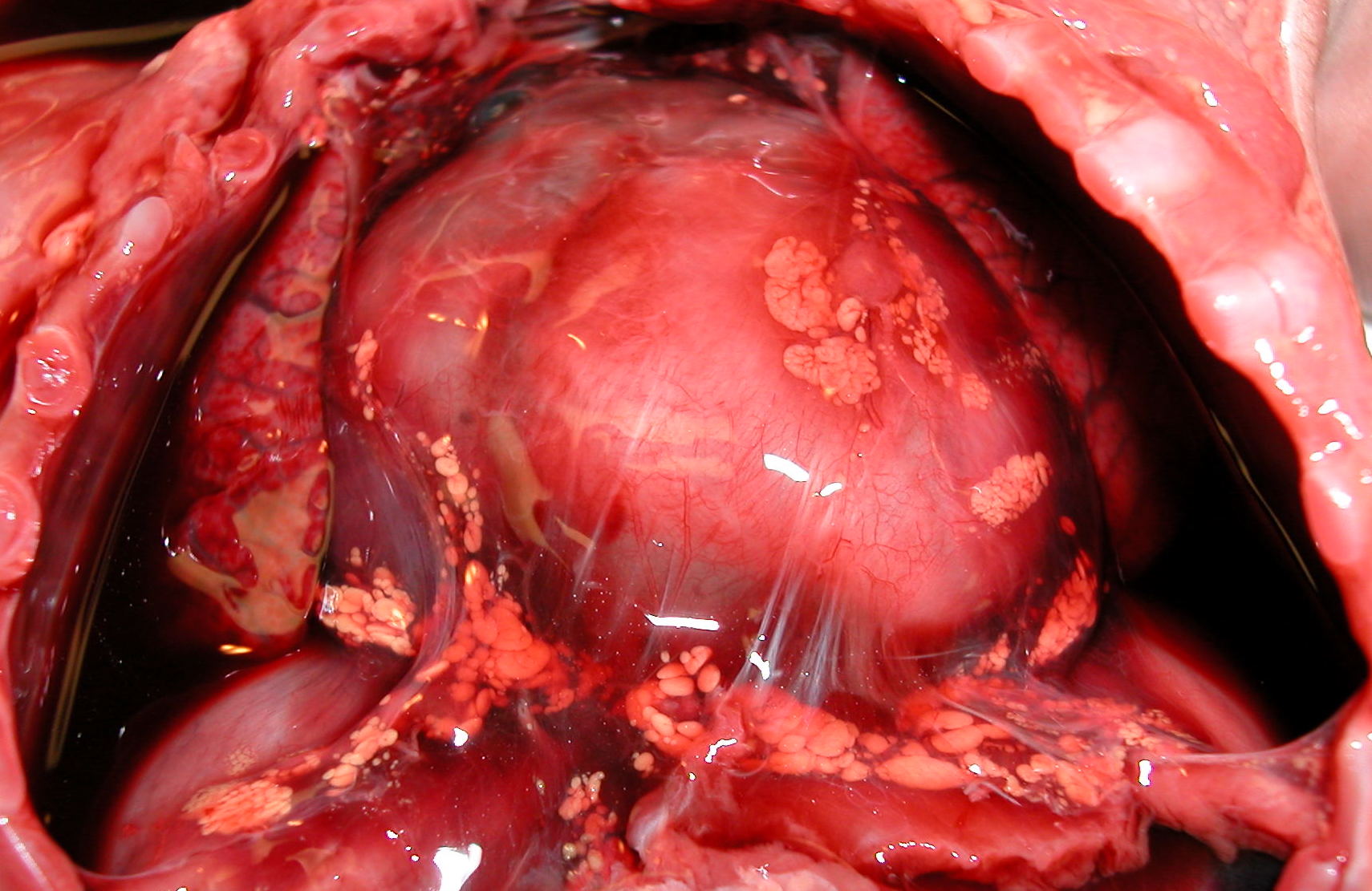
Subcapsular Hematoma: On opening the abdomen, usually in preterm infants, there may be a hematoma, usually relatively new, beneath the anterior margin. The subcapsular connective tissue is weak and connected to the sinusoids as the likely source of the hemorrhage. It is possible to produce such a hematoma postmortem with pressure on the liver, and possibly some are produced by delivery trauma. However, there are factors that suggest a predelivery origin such as the association with perinatal fetal sepsis1. Occasionally they may rupture and cause a large hemoperitoneum (Fig 1).
Size: The liver may be enlarged from congestion, increased erythropoiesis, and other causes (Fig 2). The liver may be smaller in growth restricted fetuses. The liver: brain ratio is a helpful judge of size, but the cause of the increase needs to be evaluated in relation to the histologic percentages of different components. The average liver brain ratio is 0.32.

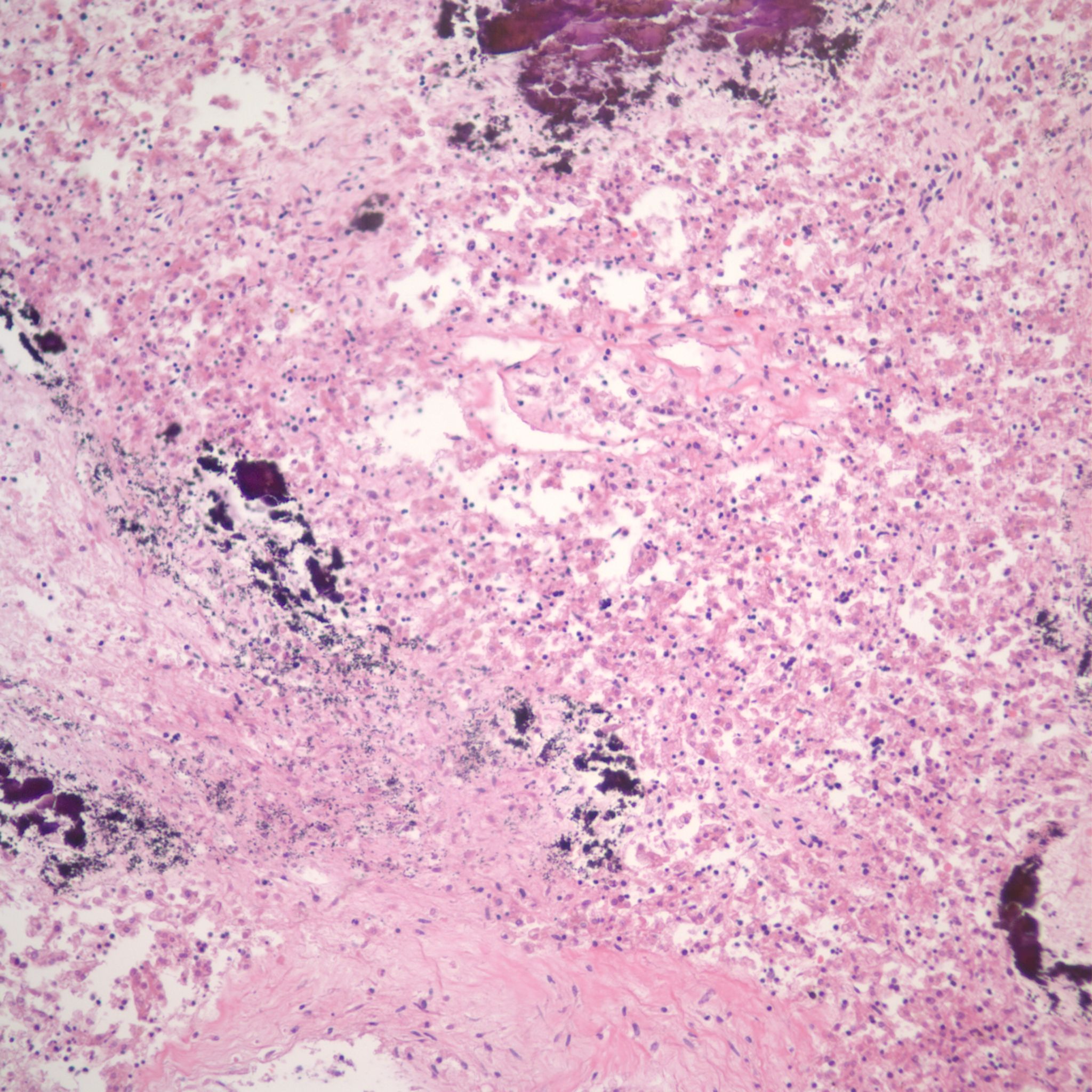
Other: Some stillborn infants usually of early gestation and prolonged retention show mineralize deposits in a branching pattern on the surface of the liver, or on radiograph within the liver (Fig 3). Microscopically these lesions stain for iron and calcium and run along the portal tracks within the liver, suggestive of old periportal hemorrhage (see below).

Sampling for histology:
Because of the asymmetric liver blood flow due to the ductus venosus left portal vein connection, cross sections from both lobes may reveal histological differences between the lobes. Lifting the liver from the abdomen will demonstrate the pale gall bladder and common duct which are not sampled if anatomically normal. Opening the internal umbilical vein into the liver will demonstrate the major hepatic vessels including the ductus venosus. The liver can then be separated from the organ block and weighed. “Breadloafing” the liver will reveal internal lesions such as hematoma or tumor.
Microscopic:
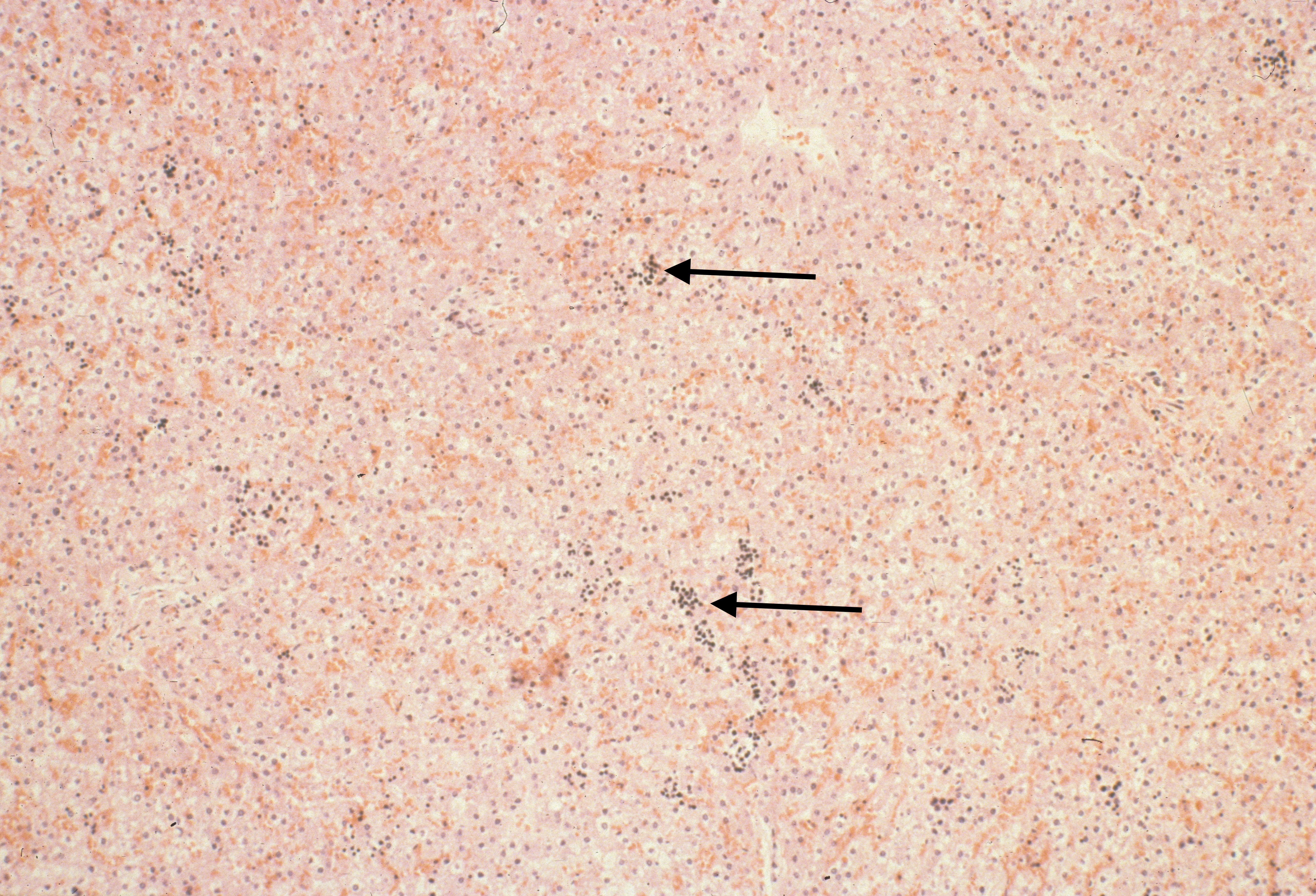
Hematopoiesis: The liver is a major site of fetal hematopoiesis. Erythropoiesis and megakaryocytopoiesis occur in the liver sinusoids. Erythropoiesis is increased with conditions requiring increased production such as fetal hemolysis or hemorrhage, and in macrosomic infants of diabetic mothers2. The extent of erythropoiesis decreases with gestational age (Fig 4a, b).

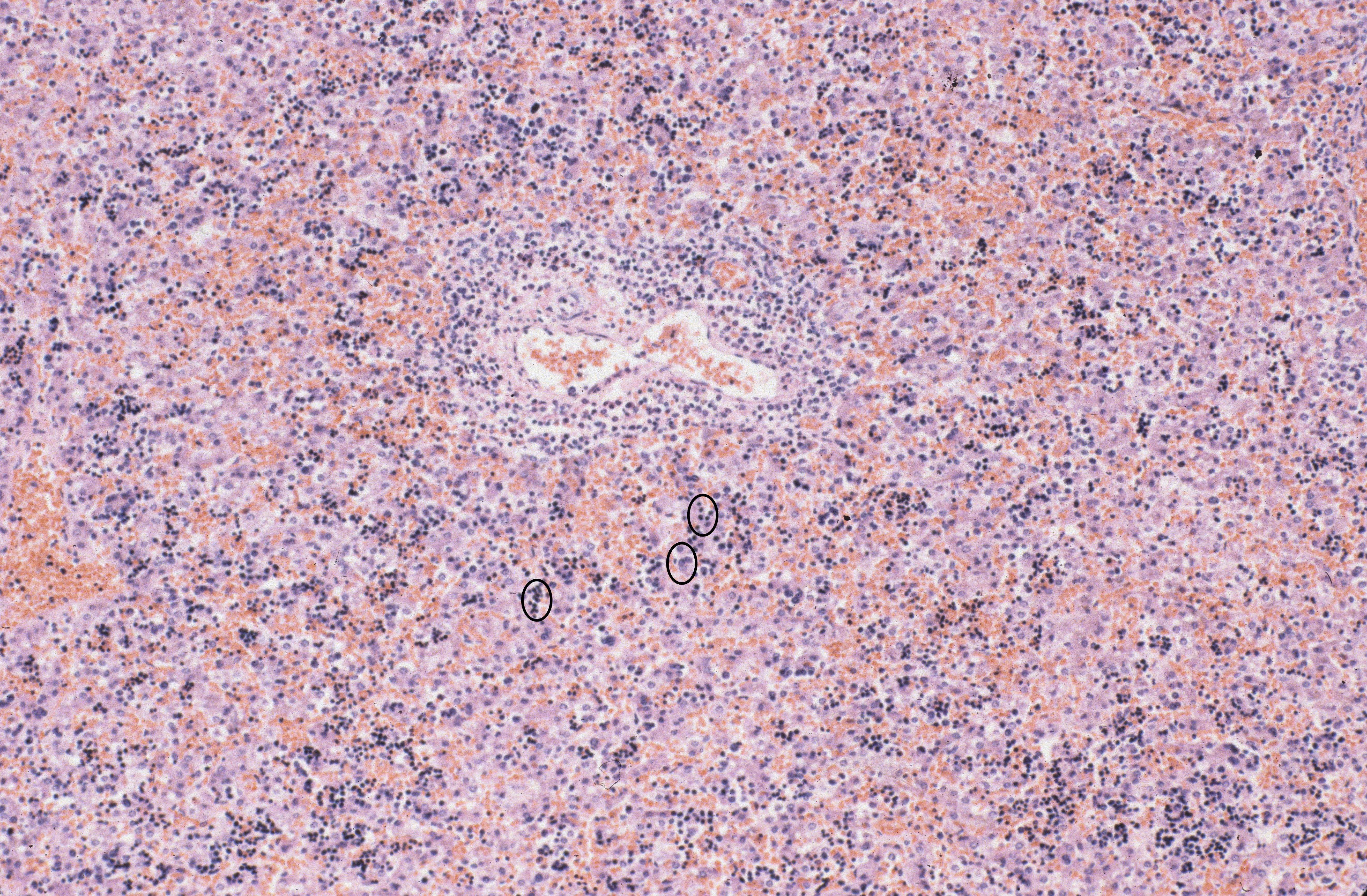
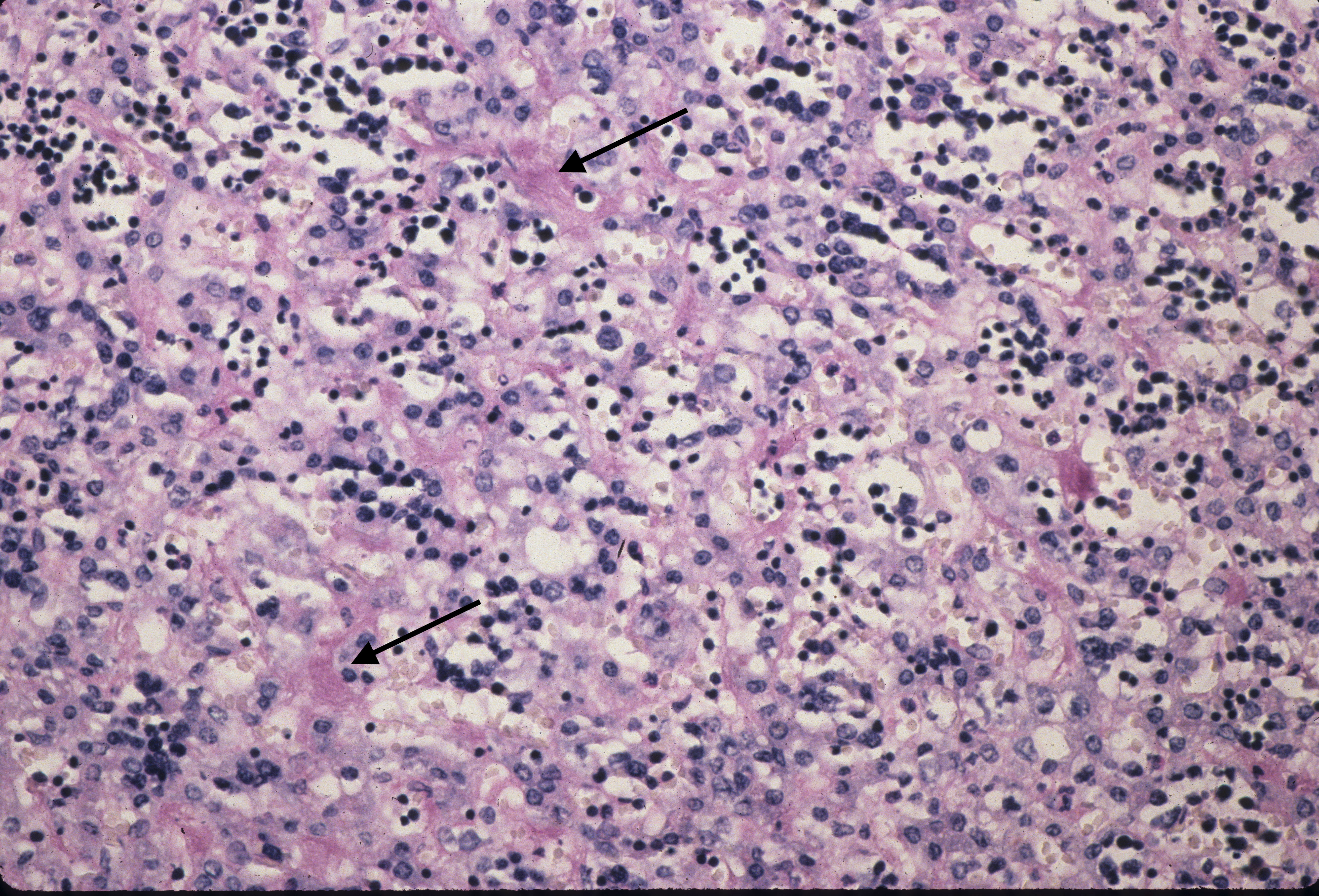
With pathologically increased erythropoiesis there is often grouping of cells at the same stage in erythropoietic development (fig 5a, b).

Increased megakaryocytes are usually an indicator of trisomy 213(Fig 6). Myelopoiesis occurs in the portal areas and may be increased with fetal inflammatory response to amniotic fluid infection4.
Hepatocytes: Liver cell disease is unusual in stillbirths. One form, gestational alloimmune liver disease, is often associated with iron storage in hepatocytes, and other organs that can accumulate iron in excess of transferrin such as adrenal and pancreatic islets5. The hepatocytes will have an increase of hemosiderin staining. Some genetic lysosomal storage diseases can cause ascites in utero6. The liver cells contain macrovesicular lipid in lethal multiple acyl-CoA dehydrogenation deficiency (glutaric aciduria type 2) (Fig 7).
Thrombi: Thrombi in liver sinusoids is a one of the lesions identified in cardiogenic shock in infants with hypoplastic left heart prior to the discovery of prostaglandin therapy (Fig 8a, b)7.

Larger thrombi in the hepatic vein thrombus which may associated with fetal ascites or fetal vascular malperfusion lesions in the placenta (Fig 9).
Hemorrhage and congestion: In the fetal liver, the majority of the oxygenated blood from the umbilical vein is supplied to the portal venous system but with a large portion also shunted through the ductus venosus to the inferior vena cava. With fetal hypoxia, the ductus venosus widens and more blood is shunted to the heart8. Despite this shift, in some stillbirths with fetal asphyxia, the liver shows marked sinusoidal congestion likely from a sudden increase in right heart pressure from cardiac hypoxia and poor contraction (Fig 10a, b).

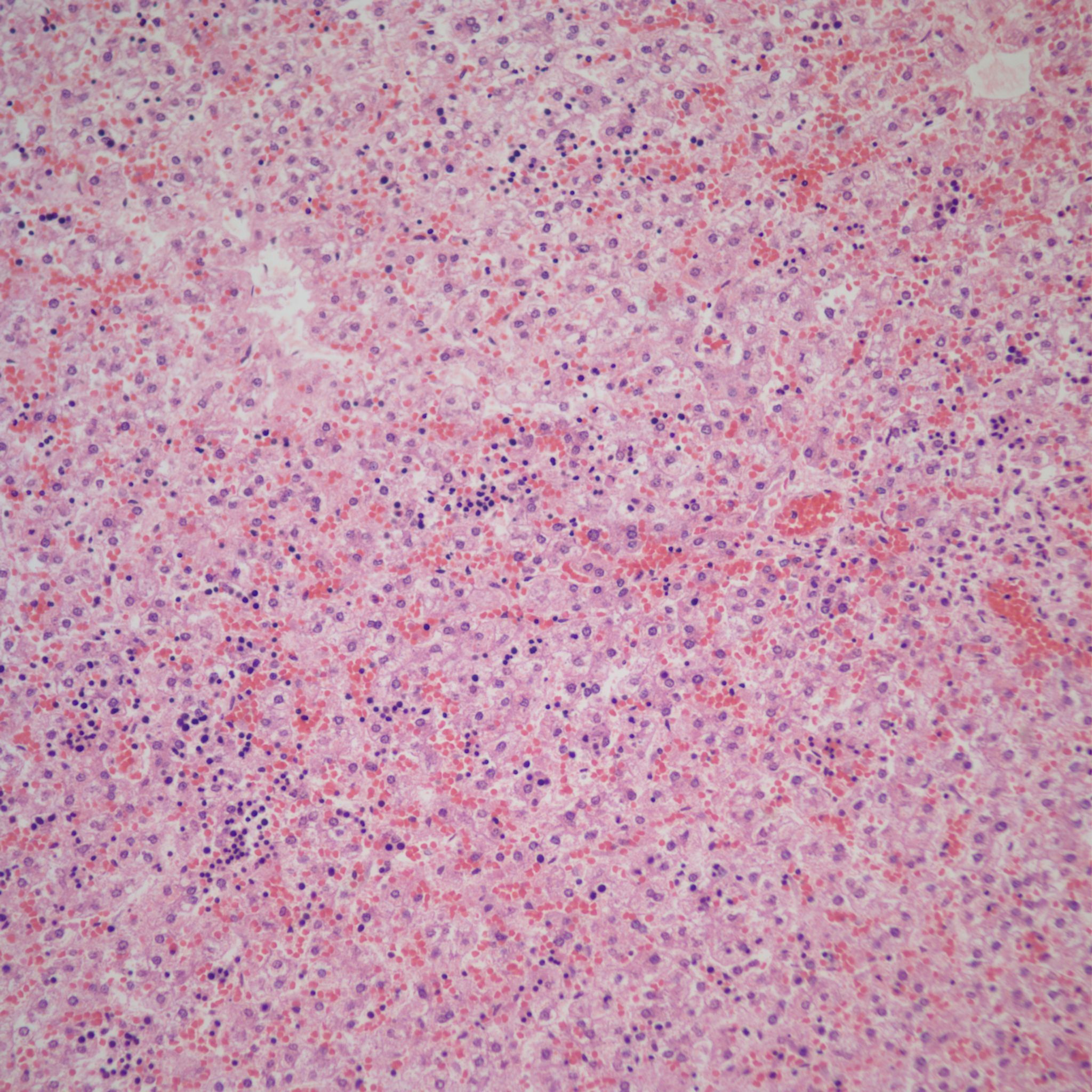
Constriction of the ductus arteriosus would also be expected to suddenly increase right heart pressure and liver congestion. The sinusoidal congestion may be accompanied by periportal hemorrhage likely because the increase in right atrial pressure is also transmitted to the portal system through the ductus venosus (Fig 11).

Because of the anatomy, such periportal hemorrhage may be more prominent in the left lobe because of the attachment of the left portal vein to the ductus venosus, but this has not been systematically investigated.
Hemorrhage can occur in the liver as in other organs with fetal septic shock presumably from disseminated intravascular coagulation, although D dimers or other evidence is not available (Fig 12).

More cryptic in origin are focal subcapsular and periportal hemorrhages seen usually in early gestation fetuses that can be seen on fine grained postmortem radiographs (Fig 13a)9. These lesions may stain for both hemosiderin and calcium. (Fig 13b, c)


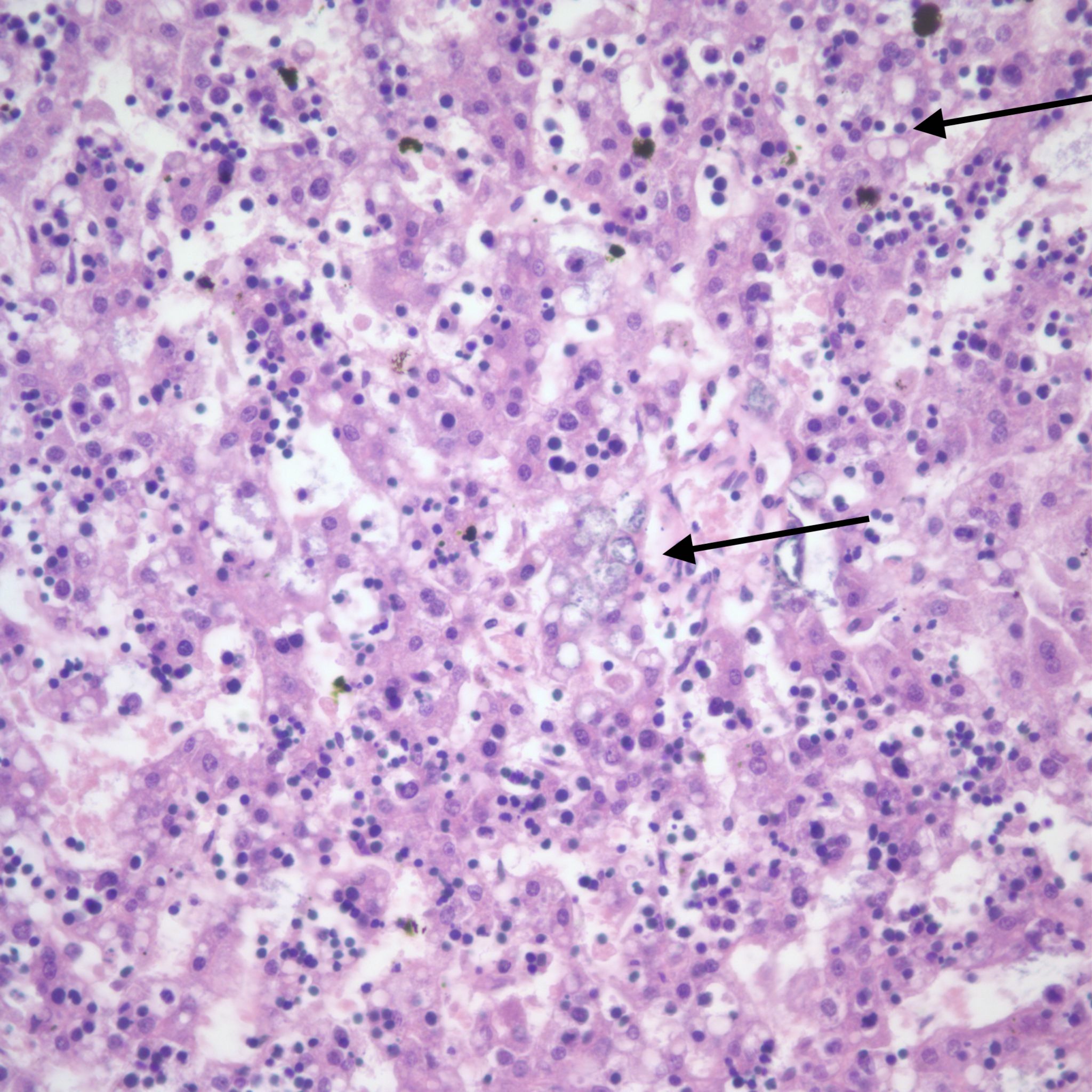
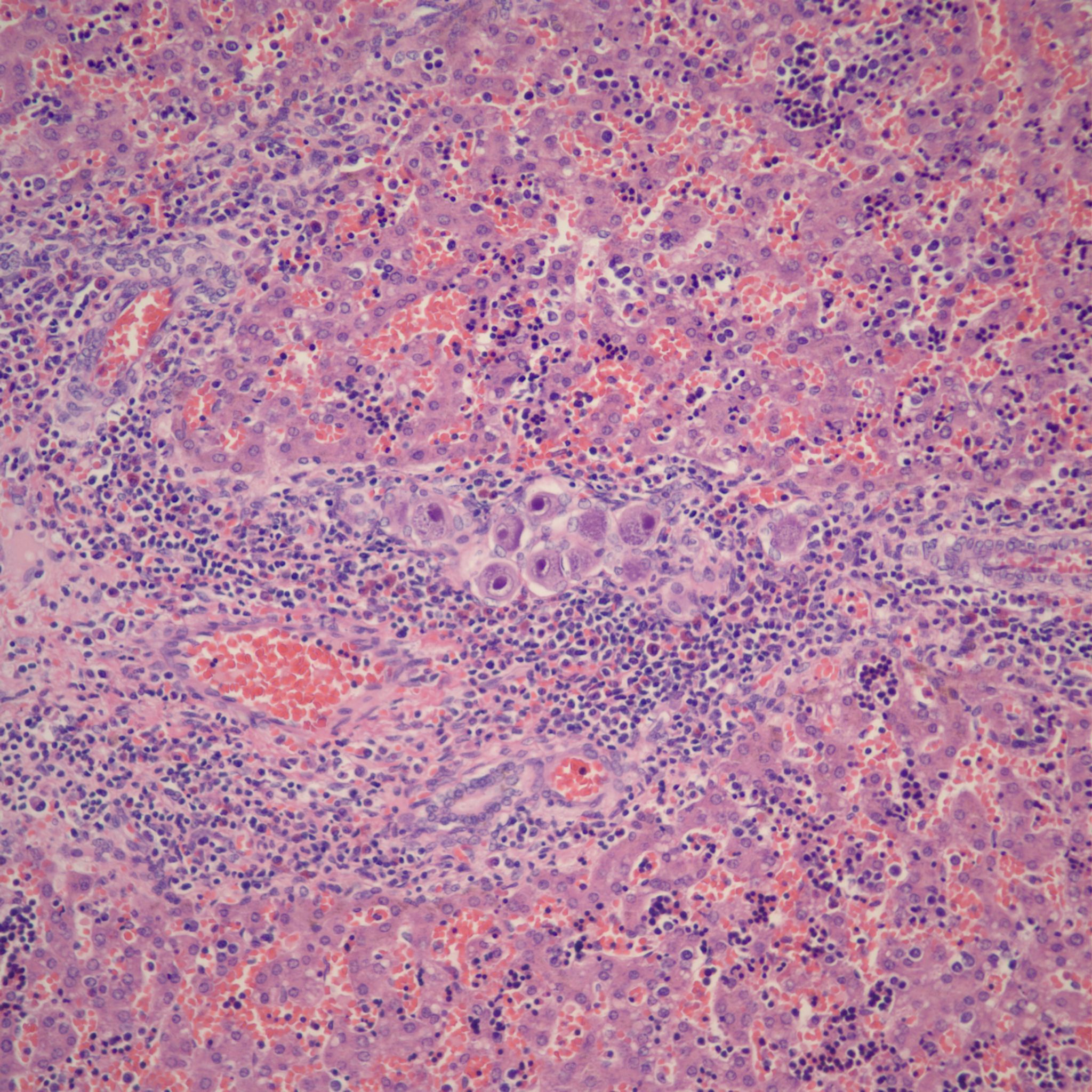
Infection: The liver cells are a prime site of Herpes simplex infection with a gross pattern of geographic necrosis. Microscopically, some cells will show typical herpetic inclusions which can be confirmed with immunostaining (Fig 14).

The portal system is a frequent site of Cytomegalovirus inclusions (Fig 15).
Other: Vascular malformations/tumors occur in the fetal period (Fig 16).
In multiple syndromes such as Infantile recessive polycystic kidneys, some short rib polydatyly syndromes, Ivemarks renal hepatic pancreatic dysplasia and Meckle syndrome, the bile ducts show a typical bile plate arrangement (Fig 17).

Duration of postmortem retention:
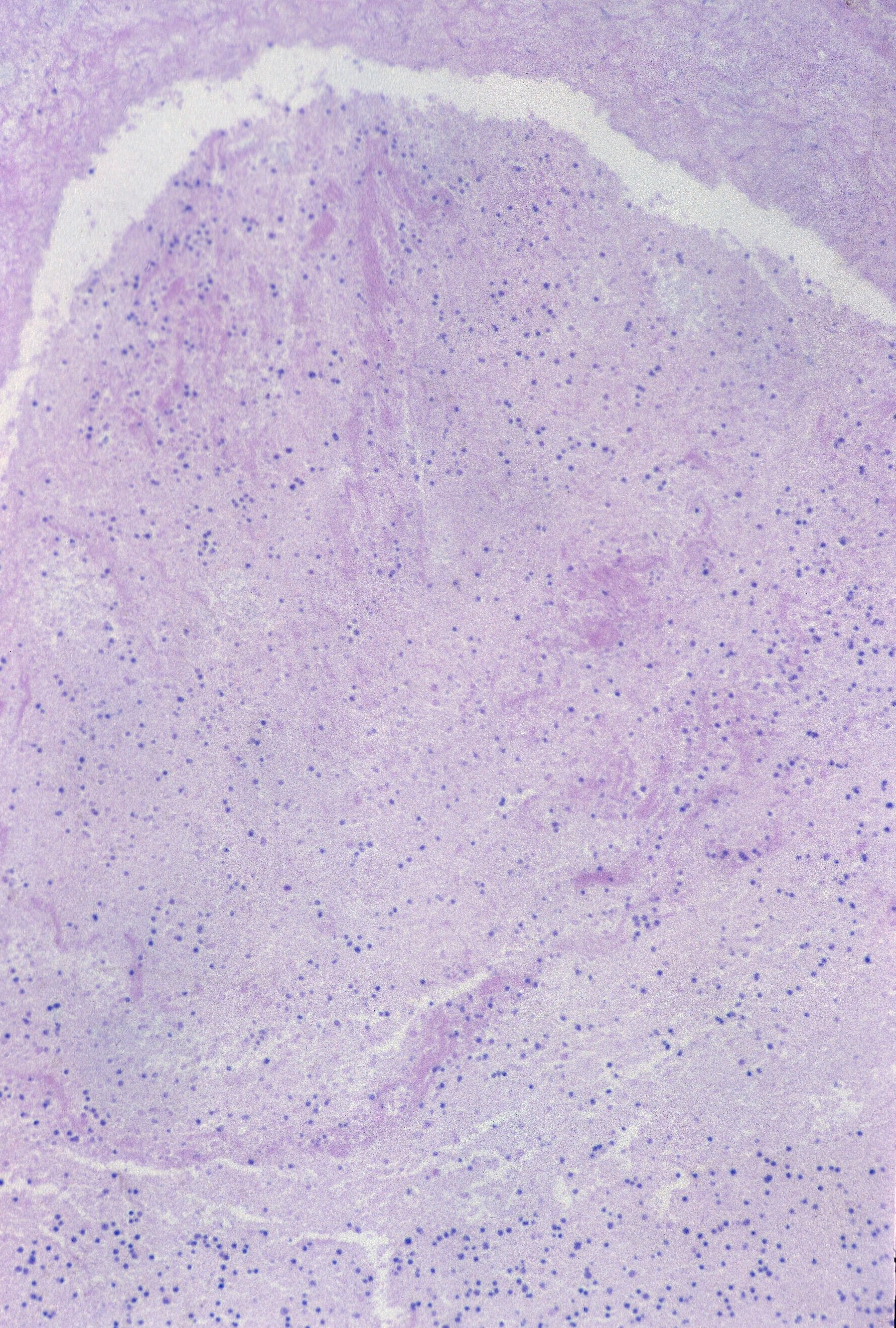
The loss of more than 1% of hepatocyte nuclear basophilia occurs in the window after 24 hours of postmortem retention (Fig 18)10.
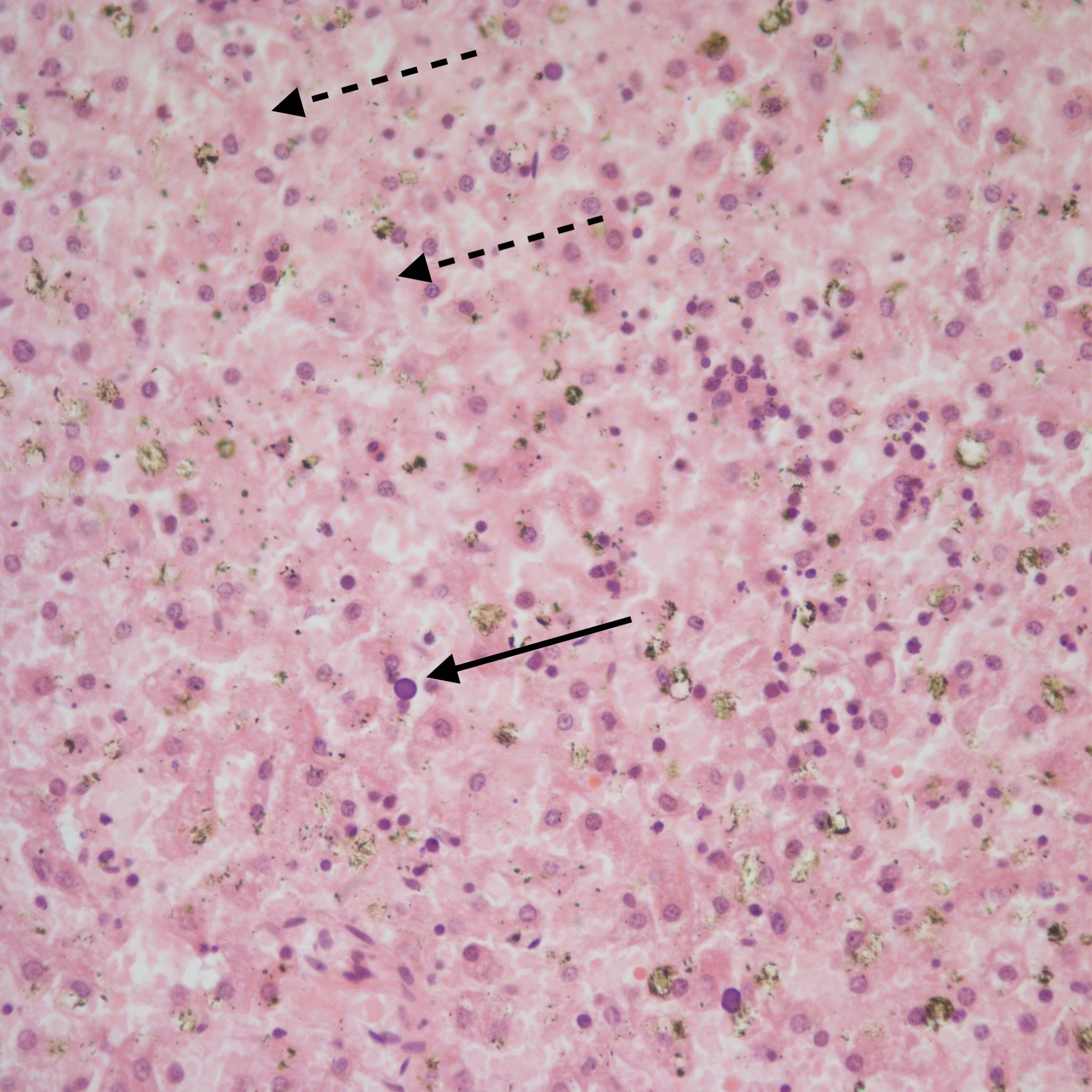
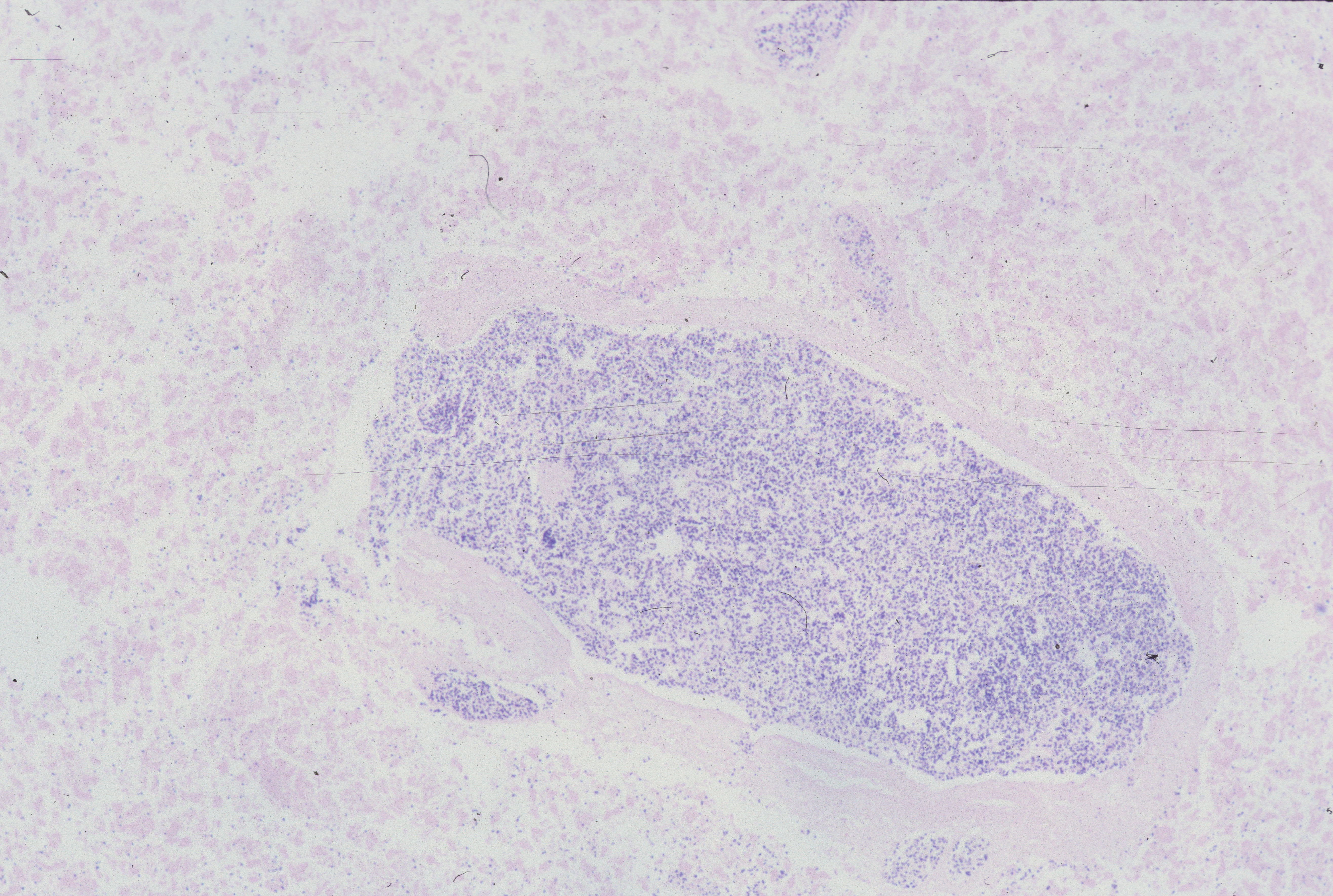
Complete loss of basophilia occurs after 96 hours. A peculiar artifact in early gestation fetuses with prolonged retention is the expulsion of brain tissue inot the body presumably during delivery through a narrowly dilated cervix. This often extrudes through the spinal foramina, but also can be driven into the venous drainage of the heart into the hepatic circulation. This artifact has been mistaken for tumor as the small blue cells retain nuclear basophilia longer than other tissues, but the diagnosis can be made by the collapse of and the loss of brain issue within, the skull (Fig 19).
1. Singer DB, Neave C, Oyer CE, Pinar H. Hepatic subcapsular hematomas in fetuses and neonatal infants. Pediatr Dev Pathol 1999;2:215-20.
2. Singer DB. Hepatic erythropoiesis in infants of diabetic mothers: a morphometric study. Pediatric Pathology 1986;5:471-9.
3. Gilson TP, Bendon RW. Megakaryocytosis of the liver in a trisomy 21 stillbirth. Arch Pathol Lab Med 1993;117:738-9.
4. Stallmach T, Karolyi L. Augmentation of fetal granulopoiesis with chorioamnionitis during the second trimester of gestation. Human Pathology 1994;25:244-7.
5. Whitington PF. Gestational alloimmune liver disease and neonatal hemochromatosis. Semin Liver Dis 2012;32:325-32.
6. Gillan JE, Lowden JA, Gaskin K, Cutz E. Congenital ascites as a presenting sign of lysosomal storage disease. J Pediatr 1984;104:225-31.
7. Coen R, McAdams AJ. Visceral manifestation of shock in congenital heart disease. Am J Dis Child 1970;119:383-9.
8. Bellotti M, Pennati G, Gasperi CD, Bozzo M, Battaglia FC, Ferrazzi E. Simultaneous measurements of umbilical venous, fetal hepatic, and ductus venosus blood flow in growth-restricted human fetuses. Am J Obstet Gynecol 2004;190:1347-58.
9. Bronshtein M, Blazer S. Prenatal diagnosis of liver calcifications. Obstet Gynecol 1995;86:739-43.
10. Genest DR, Williams MA, Greene MF. Estimating the time of death in stillborn fetuses: I. Histologic evaluation of fetal organs; an autopsy study of 150 stillborns. Obstet Gynecol 1992;80:575-84.
