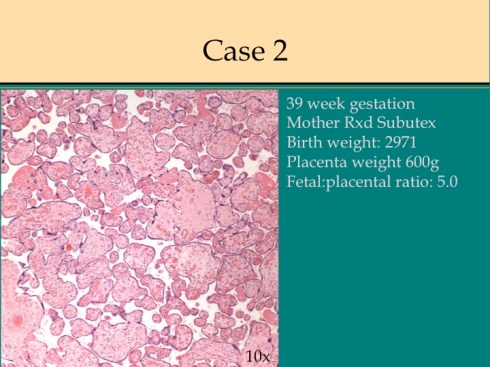
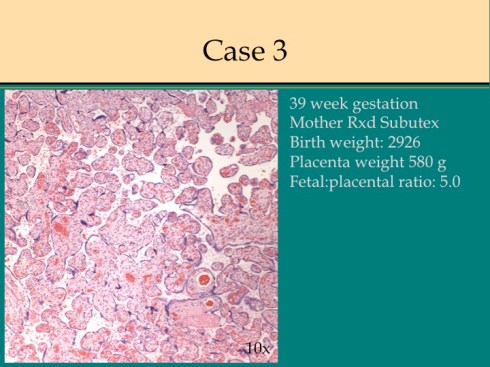
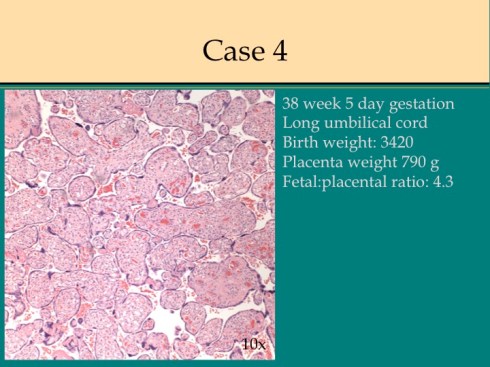
In the course of performing pathologic examination of placentas, our group noted an increase in the diagnosis of villous dysmaturity in placentas from patients being treated with Subutex for heroin addiction. We internally tested our ability to recognize the villous dysmaturity in these patients by comparing two sets of 4 placentas respectively from mothers treated with Subutex or Methadone therapy. Blinded to the clinical history, our group of pathologists consistently identified the slides from the mothers with Subutex as showing villous dysmaturity and no abnormality in the methadone group. This observation was presented at the Society for Pediatric Pathology perinatal slide review in Toronto. (see attached Powerpoint slides). At the presentation, Dr. Fusun Gundogan from the Women and Infant Hospital of Rhode Island confirmed making a similar observation. We sent this pathologist our 2 sets of test slides without any clinical history, and she also recognized villous dysmaturity on 3 of the 4 placentas from the Subutex treatment placentas and none from the methadone treated placentas.
Subutex has recently replaced methadone as the treatment for heroin addiction in pregnancy because of studies showing less neonatal morbidity1-3. The active drug is buprenorphine and there are variable dosing schedules. It crosses the placenta4.
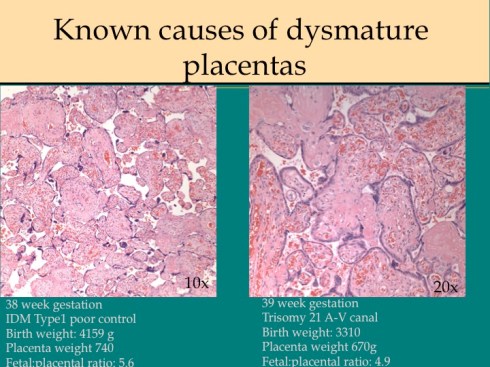
Delayed villous maturation is a somewhat subjective placental diagnosis that in our practice refers to an increased number of immature villi (large, irregular shape, with thick even syncytiotrophblast and few syncytial knots) compared to normal maturation5. The diagnosis is most often evident with aneuploidy particularly trisomy 21, and rarely with diabetes unless there is very poor glucose control. In many placentas with the diagnosis, there is no immediate clinical correlation.
The villi in the placenta mature to increase the surface area for oxygen diffusion. The rate of oxygen diffusion from maternal to fetal blood is inversely related to the third power of the barrier thickness6. Therefore maximum oxygen exchange occurs in villous areas of capillary syncytial membranes in which the fetal capillary is at the surface, and the syncytiotrophoblast is markedly attenuated. The development of such membranes is associated with the clumping of apoptotic syncytial nuclei in adjacent areas. As demonstrated by radiographic cinematography in the primate placenta, the intervillous maternal blood enters from the spiral artery in a fountain effect7. This area of perfusion from a single spiral artery has been termed the placentone8. Typically, the periphery of the flow is the first area to show placental maturation, most easily seen as an increase in syncytial knots.
Larger, immature villi have more blood vessels in the center of the villi. A placenta with fewer mature villi would be expected to be less efficient at oxygen exchange. One hypothesis for the persistent immature villi is that they are an adaptation to better intervillous blood flow such as having slower, high volume flow with better oxygen transfer. The other explanation is that there is a pathologic delay in maturation or a misreading of the normal signals that induce maturation. If the first explanation is true the infants should have normal labors because the fetus can recover oxygenation between contractions. If the second explanation is true, then some abnormalities of labor would be expected.
Women with a history of heroin addiction may be more likely than the average population to have used other drugs including alcohol and cigarettes. To test any hypothesis in this group of patients, the ideal controls would be matched for this difference from the general population. A proxy for such matching is to compare historical controls having methadone treatment. There is also a need to recognize that patient reported use of drugs and medications including Subutex may not reflect actual use.
I had considered trying to coordinate a larger study to confirm this possible association of villous dysmaturity and Subutex, but it proved more complex than I could undertake. I would be interested if any one else has made a similar observation.
References:
- Kakko J, Heilig M, Sarman I. Buprenorphine and methadone treatment of opiate dependence during pregnancy: comparison of fetal growth and neonatal outcomes in two consecutive case series. Drug Alcohol Depend 2008;96:69-78.
- Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med 2010;363:2320-31.
- Brogly SB, Saia KA, Walley AY, Du HM, Sebastiani P. Prenatal buprenorphine versus methadone exposure and neonatal outcomes: systematic review and meta-analysis. Am J Epidemiol 2014;180:673-86.
- Concheiro M, Jones HE, Johnson RE, Choo R, Shakleya DM, Huestis MA. Maternal buprenorphine dose, placenta buprenorphine, and metabolite concentrations and neonatal outcomes. Ther Drug Monit 2010;32:206-15.
- Redline RW. Classification of placental lesions. Am J Obstet Gynecol 2015;213:S21-8.
- Mayhew TM, Jackson MR, Haas JD. Microscopical morphology of the human placenta and its effect on oxygen diffusion: a morphometric model. Placenta 1986;7:121-31.
- Ramsey EM, Donner MW. Placental vasculature and circulation. Philadelphia: W. B. Saunders Company Ltd; 1980;22:26-57.
- Schuhmann RA. Placentone structure of the human placenta. Biblthca anat 1982;


Leave a comment