I have just posted as page on this site, a section on infarctions from my old web site. It asks and tries to answer a series of questions about placental infarctions*. I posted it because I found I was re-asking myself the same questions about infarctions as I pondered the excess of multiple (>2) placental infarctions in SGA stillborn infants in my autopsy database. In most of the cases, the infarctions approached but did not exceed 50% of the parenchyma, the limit that seems to be lethal in clinical abruption (Fig 1a, 1b). I was not able to evaluate in retrospect whether the areas away from the infarctions were more severely affected by uteroplacental ischemia, than in infants with multiple infarctions who did not die, or in small for gestational age stillbirths without placental infarctions. In some cases, the photographed placental slices were mixed with small retroplacental hematomas (RPH) that acutely devitalized larger volumes of placenta than the usual infarction. A perhaps instructive case was that of a fetal death, followed the next day by lethal maternal organ infarctions(1). The infant’s placenta had multiple contemporaneous, still red, infarctions (Fig 2). They involved less than 50% of the placenta. Since the mother had appeared well before the fetus died, the acute effects of the infarctions were not likely related to decreased maternal perfusion. In some of the small for gestation fetuses, the placental infarctions could exceed 50% of the volume, but they had occurred at different points in time. We don’t know the immediate effects of an infarction on the fetus but likely it depends on how quickly fetal blood flow through the dead/dying villi is occluded, as well as the overall adequacy of placental perfusion. The important question is whether ultrasound detectable infarctions can be evaluated as a separate risk factor for death in fetal growth restriction in order to prevent fetal death. For placental pathologists, the important question is how to best make our placental examinations contribute information that will help obstetricians understand fetal risks with infarction, and prevent fetal death.
Most studies of stillbirth use relatively conventional protocols for examination of the stillborn placenta and autopsy. I think these protocols are too restrictive, and that the approach should be to do “whatever it takes” to understand the full mechanism of death. The exam should sample enough spiral artery domains to gauge the overall arterial flow by quantifying villous evidence of adaptation to decreased flow. We need to sample enough spiral arteries still embedded in the basal decidua to look for patterns of disease. We need the best estimates of volume of infarctions and how they affected fetal flow and exchange over time. We need to be able to compare one placenta to another in terms of its resistance to fetal hypoxia/ acidosis for a given a degree of maternal hypoxia or uterine contraction. I don’t mean that we know how to do this now. I am trying to define a goal. I believe that goal will require synthesizing a great deal of basic science and clinical knowledge, and also a more extensive approach to placental measurement and histological sampling.
For stillbirth, postmortem fetal changes in maternal blood flow and fetal blood flow need to be considered. The best placental samples for my purpose are those with short intrauterine postmortem retention, and in placentas from infants with fetal growth restriction due to utero-placental ischemia. Normal placentas would also be needed.
Below is an imaginary approach to a thorough placental examination. For me, it is a start to thinking about a more informative approach. I would be delighted with any thoughts or experiences from readers.
The exam would start with a photograph of the fetal surface with a 1 cm grid underlay and marking of a number of marginal points needed to align the placenta to the grid. Keeping the same orientation, the maternal surface is flipped matching the marginal points and photographed. The external points can be marked with staples, suture or whatever works. The points need to be sufficient to keep the placenta oriented on the grid. Then the placenta is sliced in 2 cm thick slices parallel to one axis of the grid. (This could be done by hand with a sharp knife. An alternative is to use an electric meat slicer. For a study of placentas with maternal anti-cardiolipin antibody(2), a second hand electric meat slicer cut very uniform slices of unfixed placenta (Fig 3).) Each slice is oriented to its grid position and sampled a number of times for microscopy. The idea is to find spiral arteries on the maternal surface (and I admit I am not yet very good at this) and include them in the histological sample. On the same sample, the idea is to relate the spiral artery to the primary villous stems on the chorionic side. These stems (40-60 in number) are also hard to locate on term placenta, but making multiple contiguous blocks would allow some to be identified. The idea histological samples would have a known relationship to primary villous stems and spiral arteries. I assume in life, the placenta attempts to match fetal to maternal perfusion; therefore it matters what portion of a villous tree is in which spiral artery blood flow. This sampling technique keeps every slide oriented to the whole placenta, and to the maternal and fetal vasculature. Some sequential blocks would be cut from fetal to maternal surface, and others parallel to those surfaces to get a different perspective. Keeping slides oriented requires a convention for orienting the samples in cassettes and then on the slides to keep the grid orientations. This overkill is purely for research in a few placentas.
The total volume could be determined by planimetry of the uniform thickness slices. Infarctions could also be planimetrically measured with some error because of the change of size with depth. The full effect of the infarct could be captured by adequate sampling of the periphery of each infarction.
Once samples are chosen the histological analysis is key and my thoughts are still in progress. This analysis needs to be more than random morphometry**. There is still value in counting knots, cytotrophoblast, vascular profiles, etc. in terminal villi, but we might be able to factor in distance from a spiral artery or level in the villous tree. Counting villous syncytial membranes is likely a good measure of oxygen carrying capacity. The work of Mayhew and that group suggest that the distance between the fetal and maternal blood flow is the most critical factor in oxygen transfer, related in to an inverse third power diffusion equation. Another possible approach is to project the outlines of villous structures onto a cellular automata grid, then using red of oxygenated, blue of for deoxygenated blood, and having the maternal at time 0 red, and the fetal blood as blue, then running a program that tries to capture diffusion and flow, the color of fetal blood in the stem veins after so may iterations may be a good measure of placental respiratory capacity for a given region. Of course, if immunochemistry could provide even more information using markers for cell cycle, growth factors, etc.
* The list of new questions, that were really old.
1: How/why do infarctions form
Usual Virchow triad in spiral arteries?
Unique transition from endothelium to trophoblast?
Where in the artery are they initiated?
Separate from small RPH or marginal separations
2: What happens in the placenta to prevent continuous fetal perfusion of the infarction?
3: What effect does an infarction have on the fetus?
Separate or with general UPI?
Timing and extent?
Is it worth detecting them, MSAFP, U/S?
Meaning of observation of multiple infarctions in SB ?
Can they be prevented?
** I am not a fan of morphometry, and not just because it is tedious. Random sampling of structured biological samples can be difficult to achieve. I attended a course in morphometry and read at least some of the two monographs of Weibel that I owned. I just don’t think the random sampling of rocks is a sound basis for understanding biological features. Admittedly some of the geometric interpretations were clever, and certainly not meaningless, but they seemed to give an incomplete picture of the biological environment.
References:
- Bendon RW, Wilson J, Getahun B, van der Bel-Kahn J. A maternal death due to thrombotic disease associated with anticardiolipin antibody. Arch Pathol Lab Med. 1987;111(4):370-2.
- Bendon RW, Hayden LE, Hurtubise PE, Getahun B, Siddiqi TA, Glueck HI, et al. Prenatal screening for anticardiolipin antibody. Am J Perinatol. 1990;7(3):245-50.
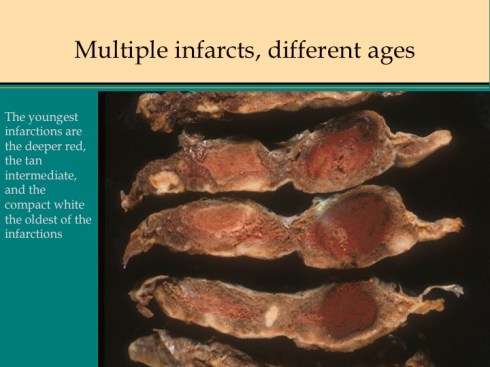
Fig 1a

Fig 1b
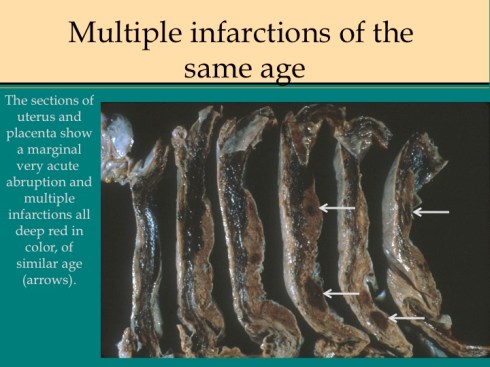
Fig 2: Multiple acute infarctions

FIG 3

Leave a comment