The “pages” that I post, review my interpretation of the published literature on a topic. Like most of us, my viewpoint is skewed by the cases I have personally experienced. I illustrate the web site “pages” with illustrations from my cases. Some of these figures evolved into short case reports that I had intended to use as addendums to the “pages”. Instead, I have given each short case report its own “page” in the hopes that it alone might tempt a reader. I have just posted three more of these reports.
As I clean up old computer files, old conference presentations, orphaned photographs, etc. I find material that doesn’t seem to merit even a short case report. I no longer have access to the microscope slides, sometimes not even to all the gross images, and no access to the clinical chart. Yet, the pieces I have still present a coherent story even if incomplete. I will pass some of these along in the blogs.
I just came across 3 microphotographs. The case presents the more usual inconclusive findings from the autopsy of a stillbirth. Now, thanks to the work of Mana Parast, Theonia Boyd and others we have one more, small piece of evidence (chorionic thrombi, FTV) that the fetal death was due to asphyxia. (Even verifying this observation sometimes requires a judgment to distinguish postmortem fetal vascular changes from pre-mortem.)
Yet, in these cases of presumed umbilical cord blood flow occlusion, we are usually missing the most critical piece of information. Where was the cord at the time of death? If only we could interest obstetricians in answering this question before delivering.
The case:
Gross Diagnosis:
- 1. Appropriate weight male infant for 26 weeks of gestation with evidence for 2-3 days of postmortem intrauterine retention.
- Mild pleural and percardial effusions
- No malformations nor evidence of infection
- Fetal thrombotic vasculopathy, pre-mortem (Fig 1,2)

Fig 1) These vilil show classic findings of HEV with an occluded lumen and extrusion of red cells and fragments.
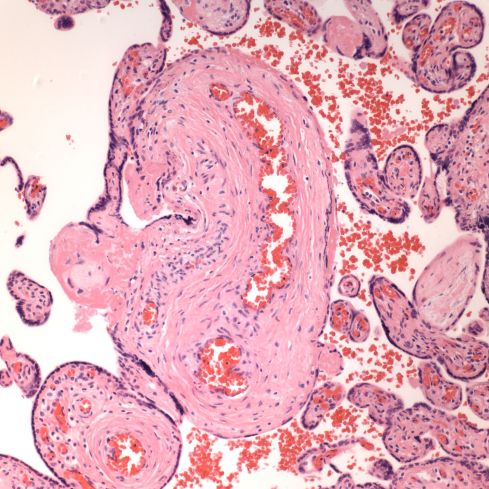
This stem villus demonstrates only recent in growth of endothelial cells from post mortem retention.
Discussion: The mechanism of death was most consistent with subacute asphyxia evidenced by pleural and pericardial effusions. This mechanism is likely related to the clinical history of umbilical cord entanglement. Entanglement may cause compromise of fetal umbilical blood flow by either causing the cord to become fixed in an area where compression can occur or as demonstrated in vitro, by causing a functional short cord due to the start of the cord wrapping near the umbilical cord insertion (J Matern Fetal Neonatal Med (2014) 27:1462).
The placenta did not show a specific cause of asphyxia. There were no fetal vascular thrombi, but there was regional variability in the timing of FTV lesions (hemorrhagic endovasculosis , avascular villi) that suggested a pre-mortem interference with umbilical cord blood flow (Pediatr Dev Pathol (2012) 15:275).

Leave a comment