I decided to restart this blog, in part to find a way to post the material that was on my now defunct web site, but also because it seems every week if not every day there is some interesting problem or conundrum in obstetrical pathology that would be interesting to share with other others with an interest in obstetrical disease. That is the blog part. The more formal material will be in the pages and starts with a few pages of historical introduction to the discovery of an association of congenital birth injury with obstetrical events.
Placental sections provide an opportunity to look at fetal blood, admittedly inferior to a blood smear. I recent interesting case in point was the placenta from an almost term infant with a prenatal diagnosis of IUGR and of hepatomegaly. The villi appeared mature, but not enough to account for the growth restriction. The villi in the center of the placentone (spiral artery flow pattern) were slightly edematous. Perhaps, that is why I looked a little more closely at the fetal blood, which appeared hypercellular. This is often the low power observation that prompts a closer look for increased nuclear red cells. In this case, there was a more or less monomorphic mononuclear cell accumulation. This observation prompted bringing up the infant’s medical record with the thought that the cells might be the result of trisomy 21. There was no indication of Down syndrome, but the total white cell count was 229,000 with 45% blasts pre therapy. The diagnosis was congenital acute B cell leukemia.
I at first was elated at having made an observation that correlated with the infant findings, but then was deflated that my diagnosis had not really added any useful information. Still, looking at fetal blood on the placental sections can add information and at the least confirm that the abnormal blood picture was congenital.
I have attached some microphotographs of the above case and other examples of fetal blood lesions in the placenta.

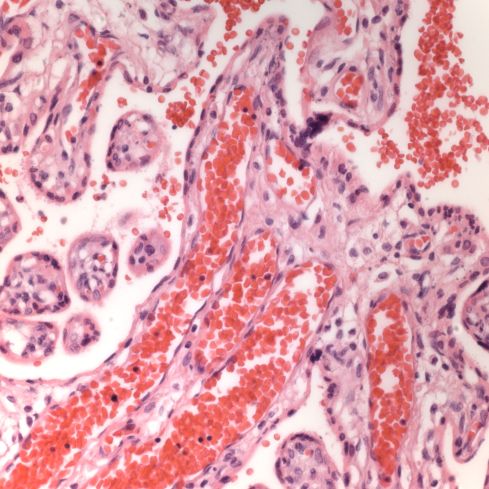
This low power image shows the increased nucleated blood cells in the stem vessel.
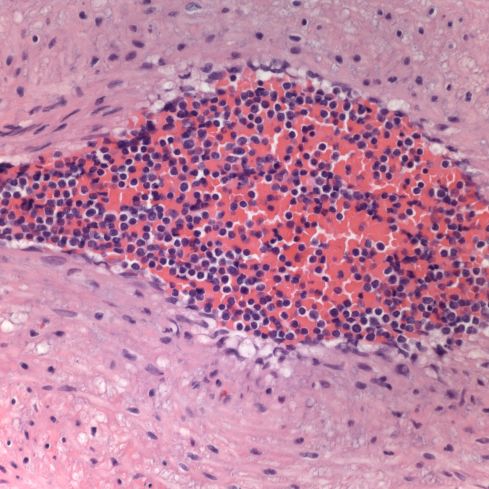
The fetal blood at first looked like increased nucleated red cells, but the cytoplasm was clear not red, and the overall impression was a monomorphic mononuclear population.
A case of familial congenital leukemia:
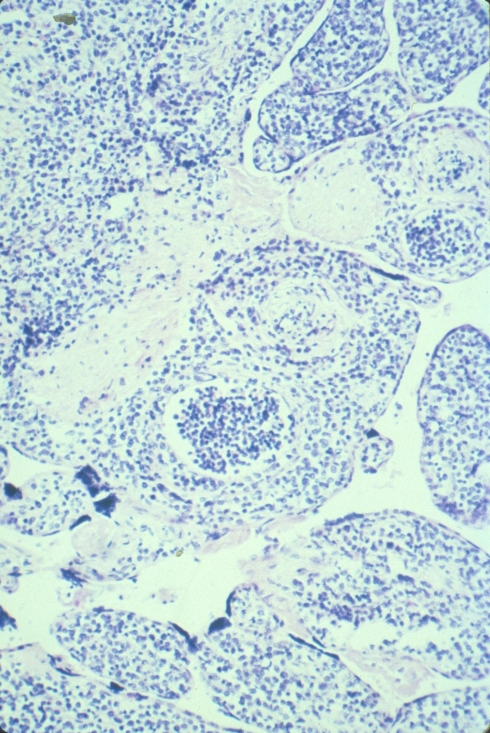
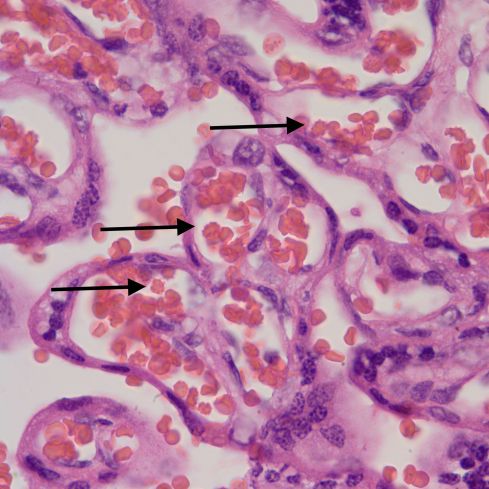
Medium power showing leukemic cells in vessels but also in the villous stroma.
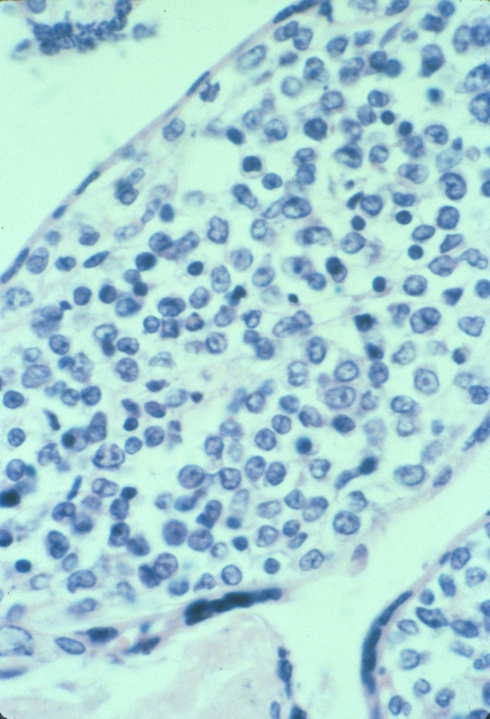
High power showing the leukemic blasts.
A placenta from an infant with karyotype 48XXY+21
This placenta had scattered possible blasts and an abnormal blood picture but my notes are missing.
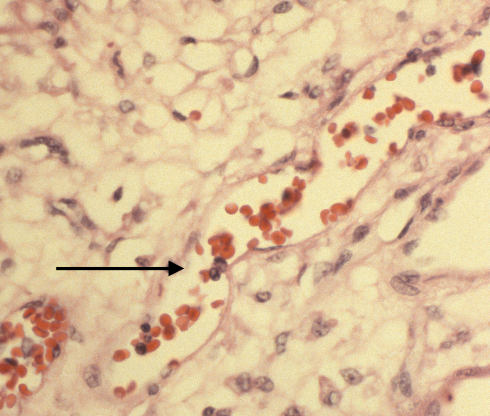
Parvo virus inclusion on H&E stain in an immuno-chemically proven case of infection.
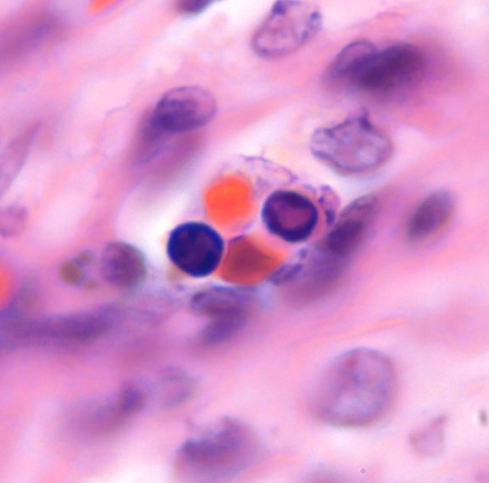
The eosinophilic inclusions of parvo virus in the nucleated red cells.
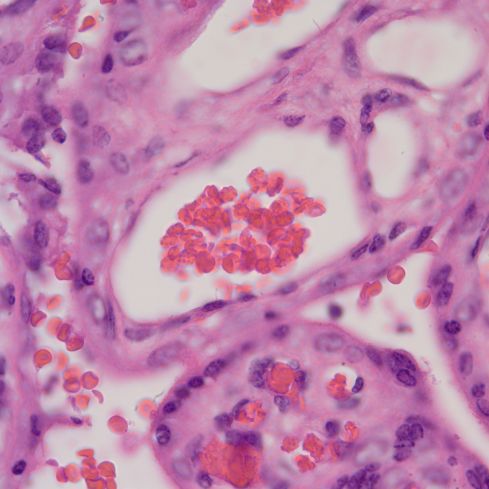
Large red cells in triploidy
The red cells are consistently larger in the fetal vessels compared to the maternal cells in the intervillous space in this 20 week fetus with dysgenic triploidy.

On this Coulter strip, the red cell population on the left from the PUBS shows the large cells. The comparison on the right is after a neonatal red cell transfusion which show the normal peak and the residual triploid population.
Acanthocytosis in an infant with absent liver apoproteins
The acanthocytes sometimes appear as knobs or as darker small spheres.
Slightly less crowded together acanthocytes.

Hi, Bob! I’m so very happy to see that you started your blog again! This one was very interesting, and perhaps it can lead into a blog on the visualization of the maternal blood from examination of the placenta… if you do, I have some nice photos of a microfilaria and malarial pigment in the intervillous space (IVS) for your blog!
All the best, Dave Schwartz