Because of the previous blog, a colleague Dr. Jeff Goldstein kindly shared a case of a 30 hour old infant with profound involution of the fetal zone of the cortex and prominent lipid in the permanent cortex, who died of severe congenital pulmonary malformation. The thymus did not show accelerated involution.
How is the involution of the fetal zone cortex controlled after birth? The biochemical evidence is that it ceases to function almost immediately although it takes days to weeks to demonstrate histologic involution. Some older papers suggested that HCG was trophic for fetal zone cortex, but not sufficient without ACTH to produce growth of this zone. Thus withdrawal of HCG with birth could be the signal for the involution of the fetal zone. If so there should be a correlation with Leydig cell involution which is HCG dependent (a luteinizing hormone analog). I searched my database for the lowest adrenal to brain ratio cases, and in the most extreme case, indeed there were no Leydig cells and the fetal zone had accelerated involution. This was a growth retarded 36 week gestation triplet infant without a clear cause of death at 30 minutes of life. I have no idea why this effect occurred, but these cases demonstrate that there are still mysteries to be solved.
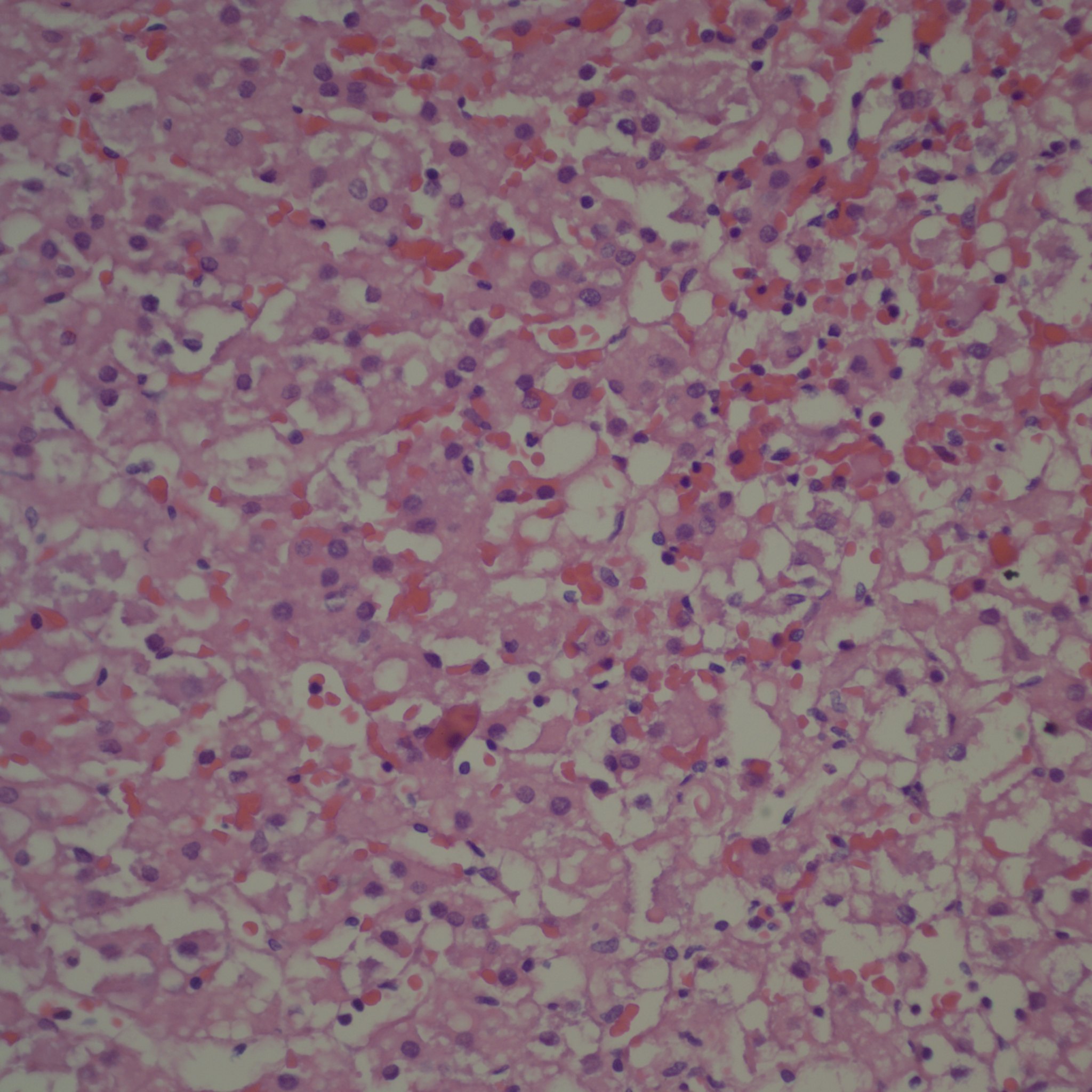
Early evidence of involution of the fetal zone 40x

Involution of most Leydig cells. 40x
However my time is finite and think I will shelve the attempt to write a book. Many placenta chapters are on my other website www.pediatricperinatalpathology.com. I also have chapters on infarction, subchorionic cysts and subchorionic thrombo-hematomas not posted. I just never found a satisfactory way to post the extensive images that I wanted to use. I think the most valuable “chapters” were on maternal floor infarctions and amnion bands because I think I was able to synthesize some material well.
Instead of the book, I have three ideas that I want to concentrate on.
The first one is that the placenta is not only an obstetrical specimen but potentially a pediatric one. This idea gained some support from the Barker hypothesis on the importance of intrauterine events on subsequent adult disease. I applied this idea to test two hypotheses to a large number of unselected placentas. The first sub-hypothesis that moderate to severe lymphohistiocytic villitis would correlate with childhood autoimmune disease was a complete negative. The second sub-hypothesis was that clinically silent old marginal separations with overlying large infarctions would predict neurologic deficits. The analysis has proved complicated and is still being pursued. However, to show clinical value for the placental examination in long term pediatric care is beyond my resources, and may not be true.
The second idea is that research needs to be directed at the natural causes of fetal asphyxia. Researchers have defined the nuances of controlled fetal asphyxia, but not really the natural mechanism. An important sub-hypothesis is that wrapping of the cord around the infant makes the effective cord length the distance from the placental insertion to the start of the wrap. This can create a short cord subject to torsion or compression from the wrapping that will compromise umbilical blood flow. I have seen more than once the scenario of a fetus with progressively worrisome fetal heart rate tracing who finally develops bradycardia and is rapidly delivered only to have hypoxic ischemic encephalopathy. The obstetrician notes a tight nuchal cord. It does not take much imagination to see that as labor progressed, this short cord by compression and torsion, was limiting umbilical blood flow, and likely at the end stopped all flow. This is a fairly good approximation to the primate model of Dr. Ron Myers of partial asphyxia followed by complete asphyxia as the mechanism that produces cerebral edema and severe neurologic injury. Unlike simple acute asphyxia there may be no window to rescue once bradycardia occurs. If the short free distance of the cord was known earlier, either elective Cesarean delivery or an intrauterine snare to unwrap the cord might have prevented disaster. Unfortunately, I haven’t found an obstetrician willing to investigate the cause of fetal distress as soon as it becomes detectable.
The third idea is that we need to know the actual initiating mechanism that leads to preterm labor in order to prevent chorioamnionitis or ruptured membranes. I have discussed some of this in my blog. I am working on a device to detect the earliest change of labor as a needed first step. This idea runs counter to those who blame chorioamnionitis as the cause of preterm labor. I think chorioamnionitis is part of the mechanism. I suspect the real root of preterm labor is in mechanisms developed to abort pregnancies when the maternal investment in the fetus was going to compromise the eventual survival of one offspring. This evolutionary approach is clearly presented in the book, “ Mother Nature: Maternal Instincts and How They Shape the Human Species”, by Sarah Hrdy.
I wish I was in an institution where research in these areas was fostered, and a pathologist’s input was welcome. There may be no such place, so I will continue to try to create one.

Leave a comment