This infant was delivered stillborn to a 25 year old, gravida 3 (para 1, fetal loss 1), mother. The pregnancy was complicated by diabetes mellitus treated with insulin. On admission to this hospital, a urinalysis demonstrated large ketones and 2+ glucose. Her prenatal testing was normal. She smoked three cigarettes per day. Her previous child weighed 5lb 15 oz at birth. She had a first ultrasound at 9 weeks gestation.
The death of the infant was discovered at an office visit the day before delivery. The labor was induced. Artificial rupture of the membranes demonstrated thick meconium. The infant was delivered vaginally with a tight wrapping of the umbilical cord around the neck and trunk. Delivery was at 37 weeks of gestation.
Autopsy:
The autopsy confirmed that the male infant was below the third percentile of birth weight (1970 g autopsy body weight) for 37 weeks of gestation. The Genest histological criteria are most consistent with three days to less than 1 week of intrauterine postmortem retention. There was still a thick layer of subcutaneous adipose tissue for the body weight. The degree of tissue autolysis made evaluation of the pancreatic histology impossible. The heart was disproportionately heavy compared to other organ weights. Erythroblastosis was present (Fig 1). The findings are consistent with the diagnosis of an infant of a diabetic mother.
There were multiple infarctions in the placenta (fig 2). As noted in a previous blog, in my experience the most common finding in small for gestation stillborn autopsies is multiple placental infarctions. My inference from this observation is that not only are these infarctions evidence of utero-placental ischemia (which accounts for decreased fetal growth), but that they also are a marker of an additional disproportionate risk of fetal death. Often there is a relatively large and recent retroplacental hematoma with overlying infarction as seen in this autopsy, and this event may be a final push to hypoxic heart failure in a compromised infant. However, a second factor in this infant is that the mother was ketotic, and if the infant already had some degree of hypoxic induced lactic acidosis, the combination may have led to increased fetal acidosis and heart failure. Either scenario, or both together, are consistent with the dilated heart and pleural effusions present at autopsy.
Gradual heart failure fails to explain the neuronal necrosis present in the basis pontis, Sommer sector of the hippocampus, putamen, and lateral geniculate nucleus (Fig 3,4). Based on experimental studies, the neuronal necrosis is the result of an acute asphyxial event followed by at least hours of survival. The meconium aspiration in this infant can be a marker of acute asphyxia (Fig 5,6). Some areas of villi demonstrated red cell fragmentation in the villous stroma, but most areas did not show this change (Fig 7,8). No thrombi were seen in the three samples taken. The evidence indirectly supports a diagnosis of fetal thrombotic vasculopathy, but is not definitive. Fetal thrombotic vascuopathy has been proposed as an important marker of compromised umbilical cord blood flow. One explanation of the relationship is based on cord compromise fulfilling Virchow’s triad for thrombus formation including blood stasis and hypoxic endothelial injury (similar to sitting too long or being in a cast).
This infant at delivery had extensive umbilical cord wrapping that could have been the basis for reduced umbilical cord blood flow. A medical student and I demonstrated in vitro, that cord wrapping can leave only a short segment of free umbilical cord (between the last point of wrapping and the placenta) that is more vulnerable to torsion induced umbilical venous occlusion. The cord wrapping provides reasonable mechanism of asphyxia. A complete unremitting sudden asphyxia would not have resulted in the neuron lesions, nor likely the dilated heart and pleural effusions, but an intermittent cord compression could produce the lesions found in this case.
Another finding in this case is the unilateral renal vein thrombosis (Fig 9). Renal vein thrombosis is more common in IDM autopsies (possibly related to osmolar dehydration in the kidney?). However, multiple placental infarctions can occur with maternal thrombophilia. In this mother there was no thrombophilic testing. A contributing role for maternal or fetal thrombophilia cannot be excluded.
Two small anomalies in the organ weight data appear to be explained by the histology (Figure 10). Normally in a very small infant from utero-placental ischemia, the thymic weight is relatively low, but it was not in this autopsy. The microscope slide shows marked lobular involution as expected, but also a large amount of non-thymic tissue included on the slide, and presumably this tissue increased the weight of the organ (Fig 11). The lungs in this case were relatively heavy, which can occur with laryngeal atresia but in this case appears most likely due to the large amount of aspirated meconium/vernix (Fig 6).
There are multiple potential causes of death in this small for gestational age infant. Subacute or intermittent asphyxia from cord wrapping is the most likely immediate cause of death, but the multiple placental infarctions, utero-placental ischemia, and maternal ketosis may have been contributing causes.

Figure 1 chorionic blood vessel: There are numerous nucleated red cells
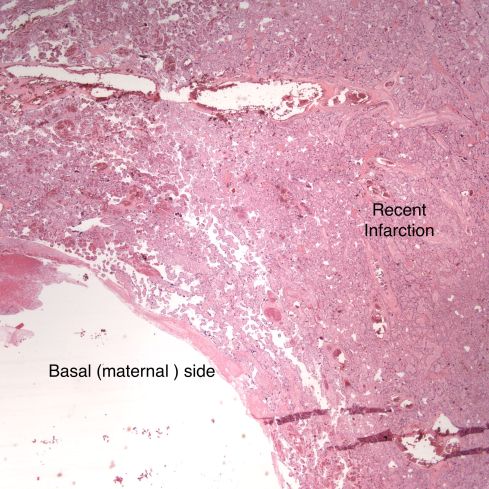
Figure 2 placenta: The right side shows compacted villi with early necrosis.
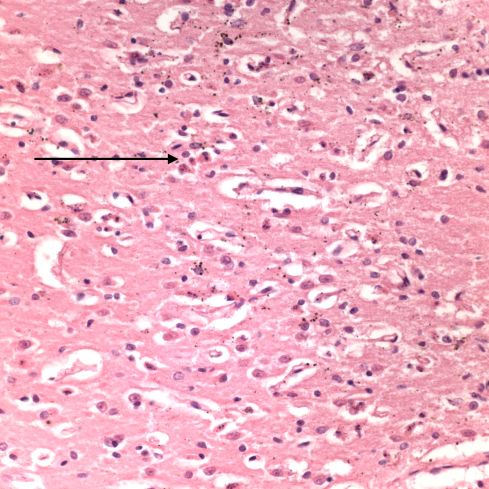
Figure 3 Somer’s sector of the hippocampus: The arrow points to one of the karyorhectic neurons which were numerous in this area.
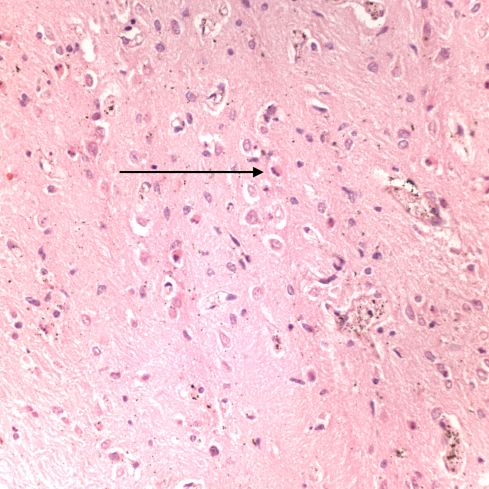
Figure 4 basis points: The arrow points to one of the karyorrhectic neurons.

Figure 5 fetal membranes: The arrow points to one of the pigment macrophages in the chorion connective tissue.
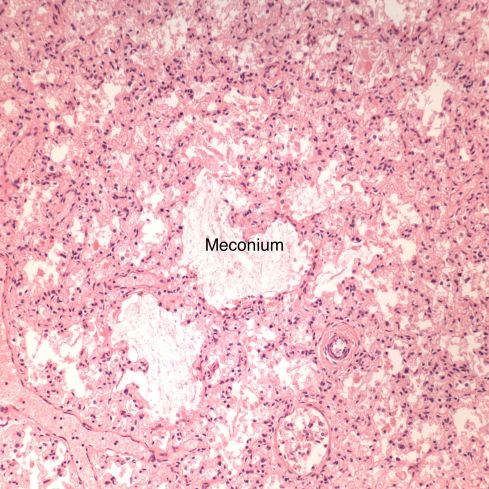
Figure 6 lung: The distal bronchioles were distended with meconium in all lung samples.
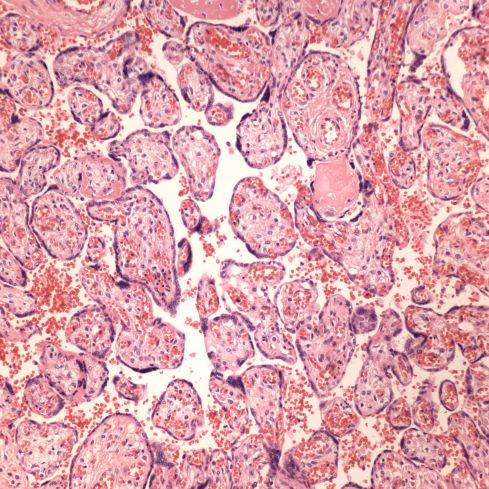
Figure 7 placental villi: These normal appearing villi composed the majority of the villi that were not infarcted.

Figure 8 placental villi: This large foci of villi demonstrates a smudged appearance of the villous stroma with extravasated, sheared red cells. This lesion occurs with downstream occlusion of fetal blood flow.
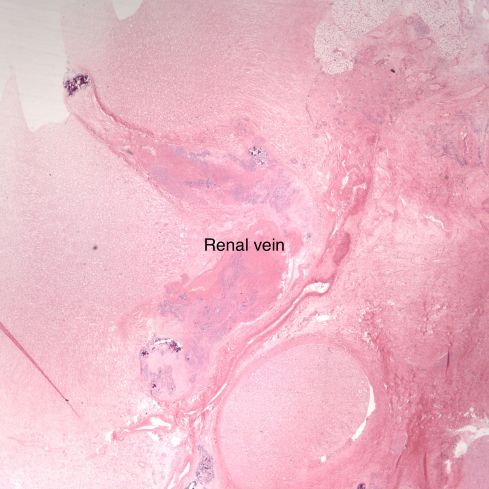
Figure 9 kidney: This low power image shows the hilum to the right with a thrombosed renal vein in the middle which is partially calcified.

Figure 11 thymus: There is accelerated involution of the lobules and muscle in the upper right corner.

Figure 10 normalized organ weights: The heart as expected was twice most of the organ weights. The lungs were almost as heavy which is attributed to meconium. The thymus was involuted and should have been smaller, but non thymic tissue was likely included in the weight.

Leave a comment