Clinical History:
This stillborn male infant was spontaneously delivered vaginally to his 26 year old, primigravida mother at 38 weeks of gestation. Four days prior to delivery, mother had reported contractions. She had not felt fetal movement for 2 days prior to delivery. An abdominal ultrasound confirmed fetal death prenatally. The mother had gestational diabetes treated with glyburide. Her urine was consistently negative for sugar on dipstick. An ultrasound at 34 weeks demonstrated an 8/8 biophysical profile, and an amnion fluid index of 20. A biophysical profile 10 days before delivery was 8/10. Her prenatal screening was normal other than glucose.
Autopsy findings:
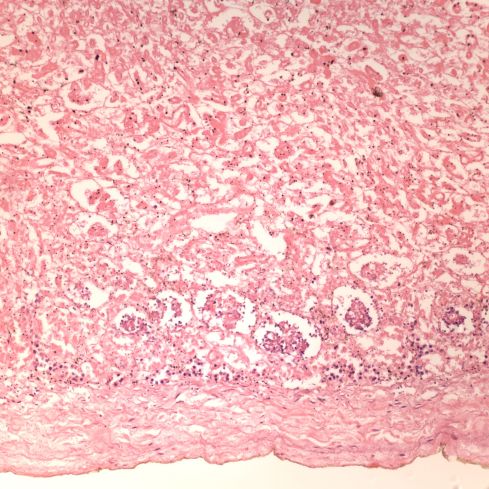
At 38 weeks of gestation the body weight is between the 3rd and 10th percentile. The placenta appears less mature than 38 weeks, the anatomic portion of the Ballard score was 36 weeks, and there may be some minimal nephrogenesis present (Figure 1). How the gestational date was determined is unknown, but it is possible that the infant is appropriate weight for 36 weeks of gestation.
The comparative organ weights do not show thymic atrophy which is expected with intrauterine growth restriction from utero-placental ischemia. The placenta does not show any significant evidence of ischemia.
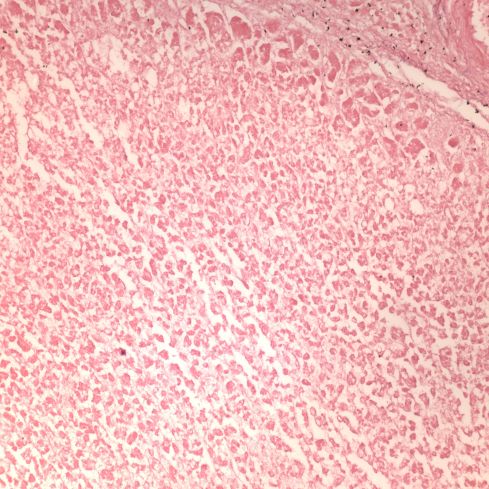
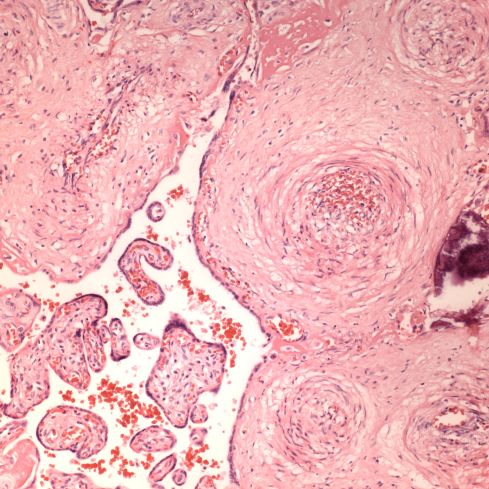
The histologic score based on Genest’s criteria would have made the postmortem retention interval between 1-4 weeks (complete loss of nuclear basophilia in the adrenal (Figure 2), and almost complete loss in the kidney). The placenta did not show similar findings but at best had endothelial ingrowth in <25% of stem vessels (Figure 3). The maternal history suggests a problem beginning with contractions 4 days before delivery and death 2 days before delivery.
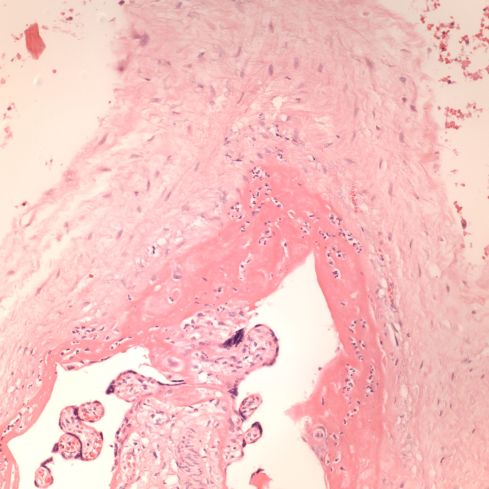
There is chorioamnionitis with a maternal but not fetal response (no neutrophils in the umbilical or chorionic vessels) (Figure 4). The postmortem lung culture was negative. There are possible gas bubbles from bacteria in fetal blood vessels in the body but no visible bacterial overgrowth. There are no neutrophils in the lung or gastrointestinal tract.
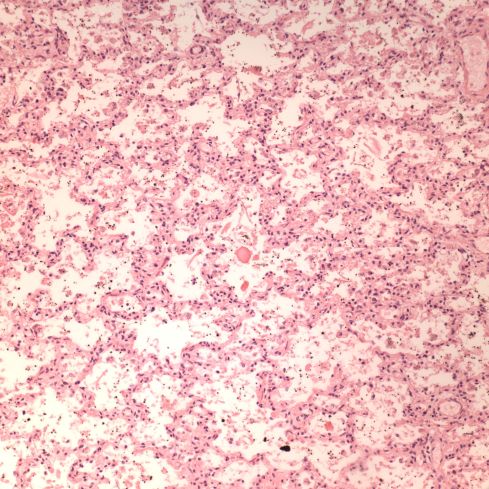
The mechanism of death appears to be subacute in that there are small pleural effusions. There are no petechiae although these can be more difficult to find with prolonged retention. There are macrophages consistent with meconium in the fetal membranes (Figure 5), and sparse fetal squames in the lungs (Figure 6). There are no airways packed with meconium or vernix.
There is little evidence of changes of the infant of a diabetic mother i.e. there is no increase in subcutaneous adipose tissue (Figure 7). The pancreas was too autolytic to evaluate. The heart was not weighed since it was fixed with the lung to dissect after fixation because of concern about abnormal pulmonary venous return, but the heart does not appear enlarged. The only evidence suggestive of maternal diabetes were increased nucleated red blood cells in the placental circulation, and these cells were difficult to identify as definitely nucleated red cells (Figure 8). The infant was not pale (anemic).
The umbilical cord length was normal (56 cm). The only placental lesion (beside the chorioamnionitis) was some mild lymphohistiocytic villitis of no significance.
Conclusion:
One hypothesis to explain the contradictions in the autopsy are that the infant was really only 36 weeks of gestation and was kept at room temperature for a prolonged period. There had been postmortem chorioamnionitis (from the fetal perspective) and some bacteria entered the fetus postmortem and contributed to autodigestion of tissue.
This leaves a 36 weeks gestation infant without evidence of the changes of an infant of a diabetic mother consistent with the prenatal negative urine dipsticks for glucose. There was some kind of subacute asphyxia with meconium passage but not gasping, and with some subacute heart failure. Thus, this infant’s death was likely unrelated to the maternal diabetes, but the cause of death remains unknown.
Enter a caption
Figure 1: Just beneath the capsule of the kidney on the bottom of the image, there is some preserved nuclear basophilia and the suggestion of a still transitional nephrogenesis. (20x H&E)
Enter a caption
Figure 2: The permanent fetal adrenal cortex is at the top. There is no nuclear basophilia. (20x H&E)
Enter a caption
Figure 3: The villous stem vessels of the placenta on the right demonstrate endothelial ingrowth, but the villi on the left are not sclerotic. (20x H&E)
Enter a caption
Figure 4: The chorionic surface connective tissue is at the top (fetal surface) and below is deep pink band of subchorionic fibrinoid with numerous neutrophils in small clusters within it. (20x H&E)

Enter a caption
Figure 5: The connective tissue of the chorion of the fetal membranes demonstrates numerous lightly pigmented macrophages. Some of these are indicated with arrows. (40x H&E)
Enter a caption
Figure 6: The lungs demonstrate occasional squames in the airways, but no compacted meconium aspiration. Such scattered squames are usually present in near term or term stillbirths. (20x H&E)

Enter a caption
Figure 8: There appears to be an increase in nucleated red blood cells (arrows) in the fetal circulation of the placental villi. If this observation is correct, it still may not be a result of the maternal diabetes. (40x H&E)
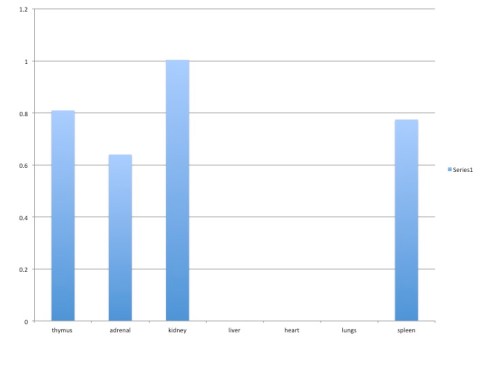
Organ to brain / average organ to brain weight graph

Leave a comment