Clinical History
The mother is a 29 year old, G2, P1 who presented following 2 days of decreased fetal movement. She has diabetes, but no other pregnancy complications. An ultrasound demonstrated fetal death with a breech presentation and decreased fluid. She underwent Cytotec induction.
Autopsy Findings:
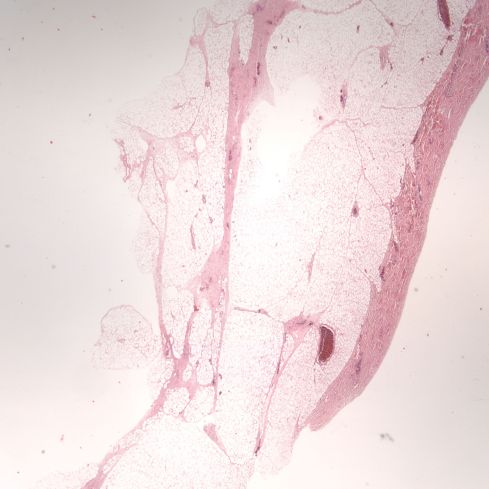
The gestational examination using the anatomic Ballard score was 33 weeks and that would place the autopsy body weight in the 75th percentile for this female infant. The heart was not disproportionately heavy. The pancreatic islets could not be histologically evaluated because of autolysis. The only evidence suggestive of maternal diabetes was the increased thickness of subcutaneous adipose tissue for gestation (Figure 1).
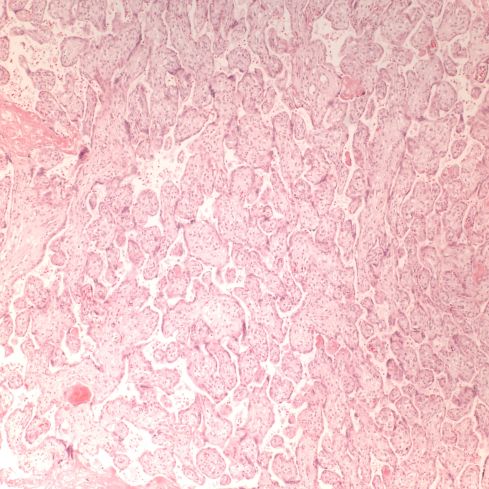
The Genest histological criteria correlated with 1-3 weeks of intrauterine postmortem retention, much longer than the clinical history (Figure 2). The placental and renal histology were consistent with the gestation (Figures 3,4). The only pathology was in the lungs which were somewhat heavy, and under the microscope demonstrated massive interstitial hemorrhage, as well as marked congestion of the capillary vessels (Figures 5,6,7). This striking finding could be interpreted as the result of premature closure of the ductus arterosis. Against this interpretation, the gross description of the heart describes only dilated ventricles and moderate pleural effusions, and the gestational age is relatively young for ductal closure. A ductus that constricts in utero typically has a wrinkled intima and at least some external narrowing, but it is possible that in a very macerated preterm infant that these features were overlooked. The usual causes of ductal closure are either oxygenation or anti-prostaglandin drugs. There is no maternal history of anti-steroidal usage, but there is very little clinical history available. Elevation of pulmonary venous pressure is unlikely to have this effect since it would likely just cause more blood to flow into the ductus instead of the pulmonary artery. There is no evidence of chorioamnionitis or pulmonary infection. The lack of meconium, and intrathoracic petechiae suggests that the death was not from sudden asphyxia.
The cause of death could not be determined, but there is no evidence that it was directly related to maternal diabetes.
Enter a caption
Figure 1: This low power photomicrograph of the skin is taken from the chest at the nipple level, the usual section location in the autopsy protocol. The deep layer of subcutaneous adipose tissue is abnormal at this gestation. (2x H&E)

Enter a caption
Figure 2: The adrenal shows complete loss of nuclear basophilia. (10x H&E)

Enter a caption
Figure 3: The subcapsular kidney demonstrates continuing nephrogenesis, an indicator of less than 36 weeks of gestation. There is still some nuclear basophilia. (20x H&E)
Enter a caption
Figure 4: The placental villi show few of the small syncytially knotted villi typical of maturation beyond 33 weeks of gestation. The villi are beginning to become sclerotic consistent with the prolonged intrauterine retention. (10x H&E)

Enter a caption
Figure 5: The lung shows massive hemorrhage in the hilum, but also there are large hemorrhages in the smaller interlobular septa, example marked by *. (2x H&E)

Enter a caption
Figure 6: This close up shows better the penetration of hemorrhage into the smaller lobular septa. The septal veins are also distended with blood. The dark granules are a formalin hemoglobin pigment that is an artifact. (20x H&E)

Enter a caption
Figure 7: At high power, the alveolar capillaries can also be seen to be filled with red cells, but due to the retention the red cells are clear. (40x H&E)

Normalized organ brain weight ratios

Leave a comment